Download
1 / 7
70 likes | 211 Vues
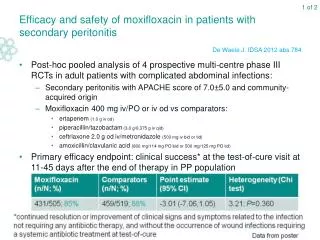
1 of 2. Efficacy and safety of moxifloxacin in patients with secondary peritonitis. Post-hoc pooled analysis of 4 prospective multi-centre phase III RCTs in adult patients with complicated abdominal infections: Secondary peritonitis with APACHE score of 7.0±5.0 and community-acquired origin

E N D
1 of 2 Efficacy and safety of moxifloxacin in patients with secondary peritonitis Post-hoc pooled analysis of 4 prospective multi-centre phase III RCTs in adult patients with complicated abdominal infections: Secondary peritonitis with APACHE score of 7.0±5.0 and community-acquired origin Moxifloxacin400 mg iv/PO or iv od vs comparators: ertapenem(1.0 g iv od) piperacillin/tazobactam (3.0 g/0.375 g iv qid) ceftriaxone 2.0 g od iv/metronidazole (500 mg iv bid or tid) amoxicillin/clavulanicacid (800 mg/114 mg PO bid or 500 mg/125 mg PO tid) Primary efficacy endpoint: clinical success* at the test-of-cure visit at 11-45 days after the end of therapy in PP population De Waele J. IDSA 2012 abs.784
2 of 2 Efficacy and safety of moxifloxacin in patients with secondary peritonitis • Overall clinical success rate: similar between groups for different infection sites • Safety analysis: Compared with other antibiotics, moxifloxacin appears to be an effective and safe option for the treatment of secondary peritonitis De Waele J. IDSA 2012 abs.784
1 of 2 Use of sonication for diagnosis of orthopaedic hardware infection Single-centre retrospective cohort study (period 2009-2011) of 48 adult patients with removal of infected orthopaedic hardware (plates, screws, nails, K wires; no prosthetic joints) Measurement of agreement (kappa statistics) between results of bacterial culture of tissue with culture of sonicate fluids from orthopaedic hardware Sonicate fluid was incubated on blood, McConkey and chocolate agar, broth media and inoculated into aerobic and anaerobic blood culture bottles Patient demographics: median age 55 yr, 30 (63%) male, 8 (17%) diabetic, 12 (25%) on antibiotics 14 days prior to culture Khumri S. IDSA 2012 abs.873
2 of 2 Use of sonication for diagnosis of orthopaedic hardware infection Sonication fluid culturing appears complimentary to tissue culturing for the diagnosis of orthopaedic hardware-associated infection but requires optimisation Khumri S. IDSA 2012 abs.873
1 of 2 Comparison of nasal mupirocin ointment with povidone-iodine solution for preventing Staphylococcus aureus (SA) surgical site infection (SSI) Investigator-driven, open-label randomised trial: 1 application nasal povidone-iodine (PI) solution vs 5-days nasal mupirocin ointment prior to surgery on SA SSI outcome in patients after arthroplasty or spine fusion surgery Standard in both groups: 2 applications of topical chlorhexidine gluconate (CHG) Endpoints: Primary: deep SA SSI at 3-mo follow-up (CDC/NHSN case definition, determined by blinded investigators) Secondary: superficial SA SSI, deep SSI due to any pathogen, drug-related AEs, risk factors for infection assessed by uni/multivariate analysis Preoperative SA colonisation associated with deep SA SSI (P=0.002) ITT analysis: 1 vs 0 superficial SA SSI for PI vs mupirocin group 6/887 (0.68%) vs 14/879 (1.59%) deep SSI due to any pathogen for PI vs mupirocin group (P=0.07) Phillips MS. IDSA 2012 late breaking abs.3
2 of 2 Comparison of nasal mupirocin ointment with povidone-iodine solution for preventing Staphylococcus aureus (SA) surgical site infection (SSI) • AE due to study drug or CHG: 3% for PI group vs 10% for mupirocin group (P<0.001) Given the lower rate of deep SSI due to SA, PI could be an effective and safe preoperative alternative to mupirocin Phillips MS. IDSA 2012 late breaking abs.3
Impact of gentamicin-collagen sponge on the risk of surgical site infection (SSI) • Meta-analysis of 14 publications/13 study populations on prophylactic use of gentamicin-collagen sponges for SSI: • Cardiac surgery (N=4) - Colorectal surgery (N=5) • Gastrointestinal surgery (N=2) - Hernia surgery (N=2) • Retrieved from PubMed/Cinahl database (period 1980-2012): data extraction independently by 2 persons, summary estimates using random-effects model The use of gentamicin-collagen sponges appears associated with a reduced risk of SSI following cardiac (but not colorectal) procedures Formanek M. IDSA 2012 abs.1294