Creating the Michigan Quality System
750 likes | 1.12k Vues
Lean Thinking in Health Care. Creating the Michigan Quality System. Jack Billi, M.D. jbilli@umich.edu Michigan Quality System: med.umich.edu/mqs. Michigan Quality System : Quality Safety Efficiency Appropriateness Service. Michigan Quality System & Lean References . 1/11/10.

Creating the Michigan Quality System
E N D
Presentation Transcript
Lean Thinking in Health Care Creating the Michigan Quality System Jack Billi, M.D. jbilli@umich.edu Michigan Quality System: med.umich.edu/mqs • Michigan Quality System: • Quality • Safety • Efficiency • Appropriateness • Service
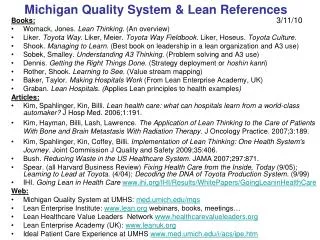
Michigan Quality System & Lean References 1/11/10 Books: • Womack, Jones. Lean Thinking. (An overview) • Liker. Toyota Way. Liker, Meier. Toyota Way Fieldbook. Liker, Hoseus. Toyota Culture. • Shook. Managing to Learn. (Best book on leadership in a lean organization and A3 use) • Sobek, Smalley. Understanding A3 Thinking. (Problem solving and A3 use) • Dennis. Getting the Right Things Done. (Strategy deployment or hoshin kanri) • Rother, Shook. Learning to See. (Value stream mapping) • Baker, Taylor. Making Hospitals Work (From Lean Enterprise Academy, UK) • Graban. Lean Hospitals. (Applies Lean principles to health examples) Articles: • Kim, Spahlinger, Kin, Billi. Lean health care: what can hospitals learn from a world-class automaker? J Hosp Med. 2006;1:191. • Kim, Hayman, Billi, Lash, Lawrence. The Application of Lean Thinking to the Care of Patients With Bone and Brain Metastasis With Radiation Therapy. J Oncology Practice. 2007;3:189. • Kim, Spahlinger, Kin, Coffey, Billi. Implementation of Lean Thinking: One Health System's Journey. Joint Commission J Quality and Safety 2009;35:406. • Bush. Reducing Waste in the US Healthcare System. JAMA 2007;297:871. • Spear. (all Harvard Business Review) Fixing Health Care from the Inside, Today (9/05); Learning to Lead at Toyota. (4/04); Decoding the DNA of Toyota Production System. (9/99) • IHI. Going Lean in Health Care www.ihi.org/IHI/Results/WhitePapers/GoingLeaninHealthCare Web: • Michigan Quality System at UMHS: med.umich.edu/mqs • Lean Enterprise Institute: www.lean.org webinars, books, meetings… • Lean Healthcare Value Leaders Network www.healthcarevalueleaders.org • Lean Enterprise Academy (UK): www.leanuk.org • Ideal Patient Care Experience at UMHS www.med.umich.edu/i/acs/ipe.htm
Background UM has problems in quality, safety, efficiency, service Problems harm patients, raise costs, frustrate workers Economy: short & long term Current state >20,000 faculty, staff, trainees >100,000 processes, all have problems Great workers trying to do a good job Goals Ideal Pt Care Experience Ideal Clinician/Staff Experience Ideal Research/Trainee Experience Safest health system in US Financial stability Analysis Workers/mgrs: +/- trained in problem solving; little std work Problems complex, cross units; work often invisible Unclear responsibility for problems Unclear priorities Time, cost pressures: stress Strategies Spread a consistent QI model across UMHS -Build on our CQI base -Study lessons from Lean Thinking 20,000 problem solvers Michigan Quality System Plan: (UMHS workers help build it) Lean Thinking in Health Care at UMHSSummary A3 J Billi 2/15/10
UMHS in a Slide Integrated Academic Health System, within major public research university: • UM Hospitals and Health Centers • 1000 beds • 1.6 million outpatient visits • UM Medical School • 1600 faculty physicians • 1000 resident physicians • 690 medical students • Total: >20,000 employees
Gaps at UMHS (and most health systems): • Quality:Not all coronary patients get statin, aspirin • Safety: • Medication errors (10x infusion pump dose) • Labs labeled with wrong patient name • Results sent to wrong clinician • Efficiency: • Nurse, doctor searching for equipment, forms, pts… • Weeks waiting for appointment to the right physician • Higher LOS: fewer admissions, less $$, lay-offs • Appropriateness: • Antibiotics for resp. infection; MRI for low back pain • Service:Patients lost, staff look too busy to help
Gaps at UMHS(and most health systems): A different perspective using lean thinking: • Waste: waiting, motion, errors -Muda • Uneven workload, variability -Mura - Busy Monday, light Friday - ORs, inpatient beds • Stress of overburden -Muri- Physicians, nurses, clerks, managers running faster- Nurse and physician shortage
Where Do We Want to Go? Our future state vision: The Ideal Patient Care Experience Based on Institute of Medicine Report “Crossing the Quality Chasm”Care that is: • Safe • Effective • Patient-Centered • Timely • Efficient • Equitable
The Ideal Patient Care Experience • The IOM “Chasm” Report gives us a vision of where to go • Lean Thinking gives us the holistic approach and business system to get there
The Ideal Patient Care Experience • The IOM “Chasm” Report gives us a vision of where to go • Lean Thinking gives us the holistic approach and business system to get there
What is Lean Thinking? Several perspectives… “The endless transformation of waste into value from the customer’s perspective”. ---Womack and Jones, Lean Thinking
Womack’s 5 Steps of Lean ThinkingApplied to Healthcare • Specify valuefrom customer’s perspective • Identify the value stream for each service, and remove the waste • Make value flow without interruptions from beginning to end • Let the customer pull value from our process • Pursue perfection - continuous improvement - Do this every day in all our activities Source: Womack & Jones: Lean Thinking
The Customer’s Perspective:Your Clinic Appointment • Call the clinic, voice prompts, on hold, leave message. • Clerk calls back and sets a date next week. • Arrive for the visit, check in, sit in waiting room. • Called into the exam room, wait for doctor. • Doctor sees you, saying she’s been waiting for you. • Diagnoses a URI, and BP is worse. • Doctor prints antibiotic prescription, walks to the staffroom to get it. You are allergic to that drug. • Doctor says to return in a week for the BP. • At check out you ask the cost – clerk says they’ll bill you, • No appointment is available next week. • Pharmacist says your insurance prefers a different drug. • Is there a problem?
Using the 5 Step Process in the Clinic Visit • Specify valuefrom customer’s perspective • A quick, effective clinic visit • Identify the value stream for this service • Request > appointment > arrival > seeing doctor > check-out …and remove the waste • Time on hold, callbacks, walking, wrong drug, unneeded test • Make value flow without interruptions from beginning to end • Staff and patient move continuously from check-in to exit • Less waiting for patient and staff • Errors surface immediately • Let the customer/worker pull value from the process • Physician pulls next patient to exam room; patient pulls med refill when needed • Pursue perfection – continuous improvement • Every day, every clerk, doctor, nurse thinks about how to redesign work to improve value to the customer, and ease for us
MedSport Appointments Long term problem: • Long delays to get an appointment • Frustrated referring physicians, patients • Frustrated MedSport staff, physicians • Incomplete records, phone tag • Physician review records prior to scheduling • Lots of hidden processes, errors, rework Project scope: • MedSport consult – from request to scheduling
Using the 5 Step Processon MedSport Appointments 1. Specify valuefrom customer’s perspective Patients, physicians and staff: quickly scheduled appointments 2. Identify the value streamfor the service Request > review> schedule appointment …and remove the waste Errors, time on hold, callbacks, physician reviews
Using the 5 Step Processon MedSport Consults 3. Make valueflow without interruptions from beginning to end Staff scheduling appointments on first phone call Uniform intake process No waiting for appointments Errors surface immediately
Using the 5 Step Processon MedSport Consults 4. Let the customer pull value from the process Same day appointments Open till 7PM 5. Pursue perfection – continuous improvement Every day, every clerk, doctor, and nurse thinks about how to redesign work to improve value to the customer
MedSport Project Results • Goal: reduce time from request to scheduling • Pre project: • process time = 27 min of work • wait time = 23 days • Post project: • 89% of appointments made on first call in 2.5 min • Physicians, nurses, and clerks: • Own the process, continue improvements • Freed to create more value • Video www.med.umich.edu/mqs
Value Stream Mapping Workshop Determine the Value Stream to be improved Value Stream Scope Understanding how things currently operate. This is the foundation for the future state Current State Drawing Designing a lean flow through the application of lean principles Future State Drawing Standardize for later improvement Developing a detailed plan of implementation to support objectives (what, who, when) Implementation Plan Implementation of Improved Plan The goal of mapping! 30, 60, 90 day follow-up From John Long
Why Draw Maps? To find problems, we have to be able to see them! • Ron Hirschl’s basement clean-up • If you make waste visible, it’s easier to remove • If you make problems visible, they’re easier to solve • In healthcare: process steps are often invisible • Hard to find the non-value added steps • We use Value Stream Mapping so we all can see the waste and find problems • How is work done now? • How could we make the job easier for workers and better for customers? • What experiment should we try first?
Value Stream Mapping:Learning to See Front-line workers: • Create the map as a team • Describe the way the work is actually done now • Not how we think it is, or how it should be… • Verify in the real workplace (“go and see”) Managers support the effort
Psychiatry Referral Process Current State Map
Value Stream Mapping:Learning to See • “Ah ha” moments: • I never knew this is how it worked! • I can’t believe what a mess this process is! • No wonder we’re frustrated! • It’s a miracle a patient ever gets through it!
Improvements don’t have to wait for workshops…We all can: • Do our work every day in a standard way that we created • Not just the way the work evolved! • Be alert to things going wrong • They always do! • Fix the problem now • For this patient or co-worker • Find and fix the root causes of the problem • So it never happens again! Modified after Spear; Billi
Lean Thinking:How To Get It “Right Every Time”Steven Spear, Institute for Healthcare Improvement • Catheter-related sepsis – a lot of little things: • No sink, no soap, no doormat reminder or buzzer • Gloves missing, wrong size, on other side of patient, at bottom of kit • 92% of nurses faced with impediments constructed ad hoc workarounds Steven Spear. Fixing Healthcare from the Inside, Today
Lean Thinking:How To Get It “Right Every Time”Steven Spear, Institute for Healthcare Improvement • Short on Time??? • Can’t find time to fix the root cause??? • Rather use a workaround every day for the rest of your career? • Just take 10 minutes a day to fix root cause of one problem • Frees up time, so next week it will be 20 min. • Then it will be 30 minutes… Steven Spear. Fixing Healthcare from the Inside, Today
Lean is not about working harder or faster Lean is about finding waste and transforming it into value our customers want.
How can we create (liberate)“20,000 problem solvers”? • Help each worker take initiative to find and fix causes of problems he/she faces daily • This means each of us has two jobs: • Do the work • Improve the work • Managers role: • Support improvement work (time, mentoring) • Align improvements so value flows to the customer Modified from J Shook
“20,000 Problem Solvers” Every worker applying the scientific method to every part of daily work. Turn all daily work into an experiment and every worker into an investigator. -Steven Spear
Scientific Method Observation Hypothesis Intervention Results/reflection Revise hypothesis New intervention… Structured abstract Lean Thinking Go see, ask why, respect Plan P Do D Check/reflect C Adjust A Repeat PDCA cycle… A3 report, Value Stream Map Lean Thinking as the Scientific Method Applied to Daily Work
Lean Thinking - An analogy to great medical care Tackle work problems with the rigor and systematic thinking we use for patient problems. Help every worker become a skilled clinician.
Lean Thinking is Like Great Medical Care for Daily Work • Great Medical Care • Collect data personally, systematically, at the bedside (H&P) • Impression and plans • Tests and treatments • Assess results & reflect • Revise impression & plan • Std write-up, presentation • Lean Thinking • Go see, ask why, respect • Plan P • Do D • Check/reflect C • Adjust A • Value Stream Map, A3
The Goal of Analysis: To Implement a Plan Determine the Value Stream to be improved Value Stream Scope Understanding how things currently operate. This is the foundation for the future state Current State Drawing Designing a lean flow through the application of lean principles Future State Drawing Standardize for later improvement Developing a detailed plan of implementation to support objectives (what, who, when) Implementation Plan Implementation of Improved Plan The goal of mapping! 30, 60, 90 day follow-up From John Long
We know half the plan is wrong, we don’t know which half. We have to watch it unfold, find what’s not working right now, and fix it. • Traditional companies think of a plan - as a prediction of what will happen. • Lean companies think of a plan - as an experiment to be conducted - to tell us what we didn’t know about the work • Paraphrase of Steven Spear , Fixing Healthcare… HBR’05 Plans are useless, planning is essential. (Eisenhower)
Can You Find Waste in Your Area? How Do They Build On Each Other? Waste? (muda) • Overproduction and Production of Unwanted Products: • Material Movement: • Worker Motion: • Waiting: • Over-processing: • Inventory: • Correction of defects: • Wasted creativity of employees: Variable Workload? (mura) Overburden? (muri)
Not All Waste Is Equal • Production of Goods, Services Not of Value to the Customer • Most important form of waste • Worsens all the others • Appropriateness – key to quality health care! • Eliminate tests, treatments, steps, processes that do not add value • Better to eliminate work than to improve how it’s done • Hard to beat the efficiency or safety of a cardiac cath that’s not done because it wasn’t needed! • If its not worth doing, its not worth doing well. • -Donald O. Hebb
Role of the Leader in a Lean Organization Standardized Problem Solving • Go and see • Ask “why?” 5 times • Respect people - Fujio Cho, Chair of Toyota Leader’s role is to mentor by asking questions - John Shook, LEI
“But we don’t have the right culture to do this…” “Act your way to a new way of thinking”. ---John Shook, Ph.D. Author, Learning to See and Managing to Learn Lean system empowers by cascading responsibility: • Standard work created by workers • Stop the line (andon cord) for abnormalities • Standard workplace to do the job every time (5S) • Systems to replenish what’s needed (kanban) • Value stream mapping to see complex processes • Structured problem solving and idea presentation (A3)
Why UMHS Chose Lean Thinking? …to improve quality and efficiency, to reduce errors and stress • It is a learning approach • Empowers workers to redesign their work • Uses “Work as Learning” • It is the scientific method applied to all we do • Uses “Work as Discovery” of new knowledge
Is Lean Thinking just CQI/TQM in a new coat of paint? Builds on Traditional CQI: • Frontline workers redesign the work • Analyzes root causes of problems (5 whys) Expands on CQI: • Starts with value defined by the customer • Each step to produce only what is needed by the next one: Just-In-Time • Uses “one piece flow” to surface problems now • Focuses on overburden & uneven workload, not just waste and errors • Value stream maps are very useful for invisible work of health care
MQS Learning Projects • Why use them? To Learn! • Goal of “Projects”: • Teach managers and workers that they can design their work to solve problems • Why not train all managers and workers first? • We Learn Lean Thinking By Doing • “Learn-do-reflect-discuss” cycle of a learning organization
MQS Learning Project Results Radiation Oncology(over 70 faculty & staff) • Patients referred for brain metastases required 3 visits over 5 days (consult, simulation, treatment) • After mapping the process, the team redesigned the process, removing unnecessary steps • Now 95% of patients have all 3 parts within 24 hours • Billing process first-time-quality increased0% to >95% • Video www.med.umich.edu/mqs
MQS Learning Project Results Results Reporting~ 13% lab results had no ordering physician, radiology requisitions lost, extensive rework • Preprinted labels (12/06) • Imaged requisitions increased by 880% (from 957 to 9380) • Labs without ordering physician fell from 13% to 2%
Goal Improve delivery of test results Accomplishments Enhanced & implemented Results Inbox Reduced lab requisitions with no ordering provider from 13% to 2% Internal Results Reporting
MQS Learning Project Results Emergency Dept. and CPU • Acute coronary syndrome: • Goal is “Door to Balloon” within 90 min. • Go and see, mapping: time spent on EKG, serial paging • Redesign patient flow, parallel paging • Within 90 min. – Increased from 75% to 85% • Time to ED discharge decreased 10 minute Before, nurses prioritized sickest, never got to discharges.
MQS Learning Project Results Care Transitions: MFH discharge from 5B • Timely appointments in hand at discharge • Management until the first follow-up visit • Mapped the discharge process, MLine pilot • Pilot results: • Decreased 14 day readmissions by 33% • Decreased visits to ED within 72 h. by 81%