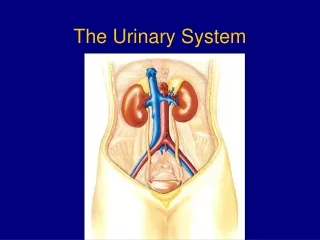
THE URINARY SYSTEM
THE URINARY SYSTEM. Kidney Stones. Renal stones: Chemical analysis can indicate why they have formed Oxalate ïƒ usually hyperoxaluria , low magnesium and vitamin B6 levels Uric acid ïƒ usually hyperoxaluria

THE URINARY SYSTEM
E N D
Presentation Transcript
THE URINARY SYSTEM
Kidney Stones Renal stones: Chemical analysis can indicate why they have formed Oxalateusually hyperoxaluria, low magnesium and vitamin B6 levels Uric acid usually hyperoxaluria Calcium phosphate possibly primary hyperparathyroidism or renal tubular acidosis Magnesium, ammonia or phosphate may indicate urinary tract infections Cystine rare inherited metabolic disorder cystinuria
Calcium Oxalate Uric acid
Calcium phosphate Cystine
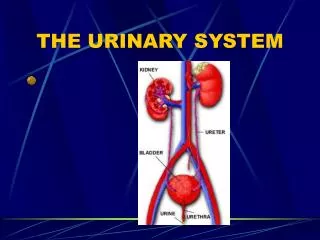
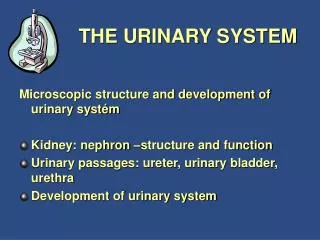
URINARY TRACT INFECTIONS
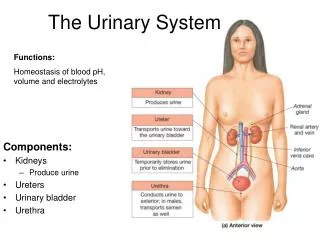
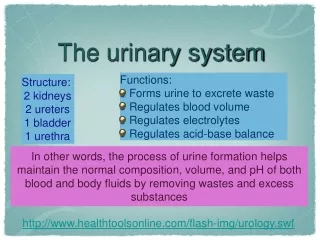
URINARY TRACT INFECTIONS Definitions • Urinary tract infection (UTI) means the finding of bacteria (or other microorganisms, such as yeasts), in bladder urine with or without clinical symptoms and with or without renal disease. It is especially common in the bladder and urethra and more common in women than men. • Uncomplicated UTI is encountered most frequently in healthy, young, non pregnant women.
Definitions • Complicated UTI refers to the presence of predisposing anatomic or functional conditions that interfere with the free flow of urine e.g. • Congenital disorders • Neuromuscular disease • Spinal cord injury • Kidney stones • Or metabolic abnormalities. This is more difficult to treat and usually requires more aggressive treatment and follow up.
Lower UTI’s refer to infection at or below the level of the bladder e.g. • Cystitis • Prostatitis • Urethritis • Upper UTI refer to infection of the urinary tract above the level of the bladder, that is • Ureters • Kidneys The term is mainly used in reference to pyelonephritis (inflammation of the kidney and renal pelvis) • Pyuria indicates the presence of pus (white blood cells; leukocytes) in the urine which may or may not be caused by urinary tract infection.
Clinical Presentation • Suprapubic pain • Increased frequency and urgency of urination • Dysuria-pain or burning with urination • Nocturia • Hematuria- blood in urine • Cloudy urine with / without a foul or strong urine odour • Upper: fever, chills, malaise, N/V, weight loss, • flank or back pain
Aetiology, Epidemiology and Risk Factors • Refer to page 515 and summarise in point form the aetiology, epidemiology and risk factors of Urinary Tract Infections (UTI’s).
Many risk factors traditionally linked to candiduria may be associated with urinary tract infections in general. Factors which predicted occurrence of candiduria, as opposed to bacteriuria, included prior use of antimicrobial agents and elevated plasma glucose. (Paul,N., Mathai,E et al. 2007, Factors associated with candiduria and related mortality’, Journal of Infection, no.55, pp.450-55)
Further Risk Factors Urinary obstruction and reflex: • Interference with the free flow of urine with any abnormality of the urinary tract such as kidney stones, creating an environment open to infection • Urinary tract obstructions can result in urine being pooled in the bladder instead of being voided, thus creating an ideal medium for micro-organisms to flourish • Reflux, which causes urine from the urethra to the bladder or from the bladder to the ureter is a risk factor in that bacterially contaminated urine from the urethral orifice can cause infection
Menopausal women • Due to a decrease in oestrogen production, menopausal women do not produce sufficient mucin to protect the bladder epithelium from pathogens. (Mucin is the protective layer that lines the bladder and postmenopausal women produce less mucin.) Women who are sexually active (especially if using a diaphragm or spermicide for contraception) • Women in the 15-24 year old age group are going through hormonal and physiological changes which can upset the flora balance in the system.
Men with prostate conditions • The prostate surrounds the urethra and with prostate enlargement and urinary stasis, it places pressure on the urethra, making urination difficult or blocking it altogether. Incomplete bladder emptying tends to favour the growth of organisms as bacteria is not flushed out of the bladder for opportunistic infection.
Researchers (www.niddk.nih.gov/health) have found that women whose partners use a condom with spermicidal foam tend to have growth of E.coli bacteria in the vagina. This occurs because: • it kills off friendly flora therefore providing the ideal environment for contamination. • It induces colonization of the vagina by E. coli and alters the overall vaginal flora. • Friction during intercourse can then force the bacteria to travel up the urethra. • UTI’s may be due to sexually transmitted diseases which are transmitted during sexual intercourse. Women are more susceptible to these because they have a shorter urethra that is close to the external environment and can therefore be more open to contamination by micro-organisms from outside influences.
Urinary catheterisation • Catheters are made of latex and plastic, and bacteria can build up as an infective film over the surface. This film can become resistant to antibiotics. These bacteria that exist on the catheter can travel up the urethra and infect the bladder. • In hospitals the primary risk factor is instrumentation of the urinary tract mainly by catheterisation. (Jensen,CS & Walter,S. 2007, ‘Urinary Tract Infections… occurrence, causes and prevention, Ugeskr Laeger, 169(49):4265-8) • Catheterization of urinary bladder resulted in urinary tract infection or colonization. Each day of urinary bladder catheterization increased the risk of development of urinary tract infection by 21.7%. (Adukauskienne,D., Kinderyte,A et al. 2006, ‘Aetiology, risk factors and outcomes of urinary tract infection’, Medicina 42(10):805-9 )
Pregnancy • Can predispose to urinary tract infections due to the normal changes in the functioning of the urinary tract such as dilation and relaxation due to: • the obstruction from the enlarged uterus • urethral relaxation caused by higher progesterone levels • The risk of preeclampsia was increased in pregnant women with urinary tract infection. (Conde-Agudela,A et al. 2008, ‘Maternal infections and risk of preeclampsia: systemic review and metaanalysis’, American Journal of Obstetrics and Gynaecology, 198(1): 7-22)
Diabetes (Geerlings,SE. 2008, ‘Urinary tract infections in patients with diabetes mellitus: epidemiology, pathogenesis and treatment’, International Journal of Antimicrobial Agents, 31S : S54 S57) • Patients with diabetes mellitus (DM) have a higher prevalence of asymptomatic bacteriuria (ASB) and incidence of urinary tract infections (UTIs) compared with patients without DM. They also more often have bacteraemia, with the urinary tract as the most common focus for these infections. • Bacterial growth in vitro is increased after the addition of glucose, however glucosuria is not a risk factor for ASB or for the development of UTIs in vivo. • Women with both ASB and DM had lower urinary cytokine and leukocyte concentrations than women with ASB without DM. As well, it was found that E. coli expressing type 1 fimbriae adhere better to uroepithelial cells of women with DM compared with those isolated from women without DM.
Treatment Protocol Antimicrobial and urinary antiseptics: Arctostaphylos uva-ursi: • Used traditionally for urinary tract infections and diarrhoea. • Has antimicrobial action against several organisms, including Bacillus subtilis, E.coli, Mycobacterium smegmatis, Staphylococcus aureus and some Shigella. It has antiseptic and astringent properties and is mildly diuretic and antilithic. Uva Ursi requires an alkaline urine to exert its antiseptic properties, so highly acidic foods should be avoided during treatment.(Heinrich et al 2004)
Maximum urinary antiseptic activity of uvaursi occurs 3–4 hours after its oral ingestion. A high intake of fruits and vegetables will sufficiently alkalinize the urine for efficacy of uvaursi in some people. (Kathy Abascal & Eric Yarnell, 2008, ‘Botanical Treatments for Cystitis, Journal of Alternative and Complementary Therapies, April, pp. 70-77) • The alkalinity required to produce the antimicrobial hydroquinone from uvaursi has raised concern that it should not be combined with cranberry, since the latter can supposedly acidify the urine to an extent that renders this hydroquinone ineffective. However, it is now known that a volume of cranberry of more than 1500 mL/day is probably needed for such urinary acidification, indicating that most people can safely use uvaursi together with cranberry. (Abascal & Yarnell 2008)
The hydroquinone generated from uva ursi has a number of potentially dangerous effects including suppression of B lymphocyte maturation and nephrotoxicity. Hydroquinone is also a known mutagen, and is one of the many toxins in cigarette smoke that contribute to cancer. This suggests that uva ursi should not be used over the long term, though the absolute levels of free hydroquinone that it generates in the urine are exceedingly small (or entirely absent according to one pharmacokinetic study in humans). (Abascal & Yarnell 2008)
Antibacterial • Refer to page 518 Enhancement of diuresis • Refer to page 519
Improve bladder function To ensure that bacteria is flushed from the bladder Crataeva nurvala • Is the best bladder tonic. • Kerry Bone (2003) lists it for: • Chronic and acute urinary tract infections. • Hypotonic, atonic or neurogenic bladder. • Incontinence. • Prevention and treatment of kidney, ureter and bladder stones.
Crataeva nurvala has anti-inflammatory and tonic effect on the smooth muscles of the bladder and the other urinary organs. This helps in the evacuation of the bladder and the control of infections. (Arora, RP., Rajiba, NL., Vineet, M., Moanty, NK., Kala, SK. 2003, ‘Role of herbal drugs in the management of benign prostatic hyperplasia: Clinical trial to evaluate the efficacy and safety of Himplasis”, Medice Update, vol.11, no.2, pp.55-58) • Crataeva nurvala is useful in the treatment of urinary disorders caused by enlarged prostate. It has anti-inflammatory, diuretic, lithotriptic, demulcent and tonic properties useful in disorders of urinary organs, urinary tract infections, pain and burning micturition. (Shukla, GN & Mahender, N. 2002, ‘Use of PR-2000, a Herbal Formulation in the Medical Management of Benign Prostatic Hyperplasia’, Indian Journal of Clinical Practice, vol.13, no.2, pp.53-56)
Improve the chronic inflammation of the bladder wall (see table 27.1) Use demulcents and anti-inflammatories It is thought that demulcent agents work via a reflex action: As they pass through the digestive tract they are believed to provoke neurologic reflexes that in turn stimulate production of mucus in the respiratory and urinary tracts. This has not been confirmed in the urinary tract, though it has been shown to occur in the respiratory tract in animals. This increased mucus production is thought to relieve inflammation and soothe pain. (Abascal & Yarnell 2008)
Improve and support immunity(Table 27.1) • Echinacea spp. • Andrographis paniculata • Astragalus membranaceous • Picrorrhiza kurroa Antispasmodics • It is generally found that when the urine is alkalised and the bacterial load reduced, the pain eases off and antispasmodics are not required.
Juniper offers a very appealing herbal “package” for patients with UTIs. Besides its potent diuretic activity, it is strongly antimicrobial and anti-inflammatory. It is surprising that all of these properties have not led to a published clinical trial of juniper for UTI. The reputation of juniper as dangerous to the kidneys is of dubious accuracy, and one text that attempted to trace the origin of this belief could find only that it was due to confusion of the essential oil of Juniperus sabina (savin) with that of juniper. (Abascal & Yarnell 2008)
Prevention:Page 519 plus (Baillie, N. 2003, ‘Recurrent Cystitis & Interstitial Cystitis’) Diet • Avoid acidic foods • Avoid foods high in sugar - chocolates, lollies, cordials • Drink plenty of fluids daily • In a study of 139 women university students, those with diagnoses of acute UTI were compared with 185 age-matched women with no UTIs in the last 5 years. • The researchers found that frequent consumption of fresh juices, especially berry juices, and fermented milk products containing probiotics was associated with a decreased risk of recurring UTIs. • Consuming fermented milk products 3 or more times per week was more effective than less than one time per week. (Hudson, T. 2006, ‘Treatment and prevention of bladder infections’, Journal of Alternative and Complementary Medicine, December, pp. 297-302)
Increasing garlic and onions in the diet—both of which produce antimicrobial activity against many organisms—may also be helpful. These two foods have been shown to inhibit the growth of E. coli, Proteus spp., Klebsiellapneumoniae, Staphylococcus spp., and Streptococcus spp (Hudson 2006) Contraception / menstruation / hygiene
Menopause • Menopausal women are more prone to UTI’s due to the ‘drying off’ of the urinary tract. • Diet high in phytoestrogens linseed, sprouts, tofu/miso, grains and such. • Trial a herbal vaginal cream applied daily or after a shower.
Probiotics • Particularly when the client has taken multiple course of antibiotics • Lactobacilli species predominate in the vaginal and urinary tracts of healthy premenopausal women. This would suggest that women who have recurring UTIs have an imbalance of their flora, and if the flora were restored, this could go a long way to prevent the infection-causing organisms from dominating. (Hudson 2006)
Back treatment • Have the back treated especially if there is any history of injury, pain and discomfort. • Practice back exercise, yoga or equivalent • Avoid wearing high heals • Impact exercise can be a trigger for susceptible women
INTERSTITIAL CYSTITIS
Interstitial Cystitis (IC) is a chronic inflammatory condition of the bladder wall clinically characterized by irritable voiding symptoms of urgency and frequency in the absence of objective evidence of another disease that could cause the symptoms • It was found in patients diagnosed with IC that 60% had only one symptom at onset, that of recurrent urinary tract infections. The study concluded that in its early stage IC manifests often as only a single state of cystitis. (Porru,D., Politano., Gerardini,M., Giliberto,GL., Stancati,S., Pasini,L., Tinelli,C., Rovereto,B., 2004, ‘Different clinical presentation of interstitial cystitis syndrome’ Int Urogynecol J Pelvic Floor Dysfunction, vol.15, no.3, pp.198-202) • Urinary frequency generally averages 16 times a day, but may go as high as 40.
In the majority of patients, IC is not a progressive disease. The symptoms do not tend to worsen with time, but tend to be intermittent. Some people have remissions for extended periods of time. • In a small percentage of patients IC can progress rapidly, causing the bladder to reduce in size and become scarred.
Pathogenesis of IC:Defective Urothelial Barrier IrritatingSolutes GAGLayer Urothelium IrritatedNerve Inflammation
IC is Characterized by a Vicious Cycle With Increased Symptomology With Increasing Age Bladder Insult More Inflammation Mast Cell Activation and Histamine Release Potassium Leak Into Interstitium Activation of C-fibers and Release of Substance P Epithelial LayerDysfunction Adapted from Evans RJ. Rev Urol. 2002;4(suppl 1):S16-S20.
Epidemiology • The non-ulcer type of IC occurs in about 90% of patients. The more severe type of the disease (in about 10% of patients) involves Hunner’s ulcers, which are lesions that appear on all layers of the bladder wall and appear as brownish-red patches on the bladder mucosa. • The ratio of females: males is 9:1. Children can also get IC • The onset is usually between 30 and 70 years and a medium of 43. • May have autoimmune cause since associated with systemic lupus erythematosis
AETIOLOGY Bladder lining deficiency • According to Baillie (2003) the most popular theory is that the symptoms are caused by some insult to the lining of the bladder, damaging the protective barrier, making it more permeable and allowing the acid urine to damage and irritate the underlying tissues. • It is this deficiency in the GAG (glycosaminoglycan-rich bladder epithelium) layer of the bladder that is suggested as the reason there is an increased incidence of related diseases. The GAG epithelium may be disrupted in patients with IC, allowing toxic substances in the urine to damage the bladder wall. This has prompted a likening of IC to intestinal hyperpermeability.
Mast cell activity • There are an increased number of mast cells and/or, increased degranulation of mast cells by excessive nerve activity that results in the release of inflammatory substances which cause pain. • 30–50% of people with IC have an excessive number of mast cells in the bladder wall (Baillie, N. 2003). • Antigenic exposure of mast cells causes a release of pharmacologically active mediators such as histamine, prostaglandins and Leukotrienes and have a significant effect on smooth muscle, vascular epithelium and inflammation.
Autoimmunity • It has been postulated that autoimmune or allergic characteristics are present in IC. • The prevalence of allergies in IC is reported to be between 40 and 80% of patients. (Van de Merwe,JP., Yamada,T., Sakamoto,Y., 2003, ‘Systemic aspects of interstitial cystitis, immunology and linkage with autoimmune disorders’ International Journal of Urology, vol.10, pp. Suppl:S35-8) • Several T cells (CD4 and CD8) were significantly more abundant within the bladder biopsies from patients with IC than controls (Christmas, TJ. 1994, ‘Lymphocyte sub-populations in the bladder wall in normal bladder, bacterial cystitis and interstitial cystitis’, British Journal of Urology, vol.73, no.5, pp.508-515). • Patients often have a history of allergies to medications and environmental stimuli, asthma, or conditions such as SLE or other immunopathologic abnormalities with a presumed autoimmune component such as inflammatory bowel disease or fibromyalgia.
GAG Bladder lining deficiency • Another theory is that IC is a defect in the glycosaminoglycans component of the mucin layer that covers and protects the urothelium. This could allow irritants to penetrate and activate bladder mast cells. • The potassium leak test was proposed as a mechanism to evaluate the status of the glycosaminoglycans layer of the bladder. This layer is theoretically lost in some cases of interstitial cystitis. When this occurs, the bladder lining becomes very irritable when exposed to high concentrations of urinary potassium. This is thought to be one mechanism by which interstitial cystitis causes pain.
The chronic pain, frequency, urgency and sleep deprivation associated with IC may contribute to psychological stress and secondary depression. Suicidal tendency is 3 – 4 times more common in patients with IC than in the general population. More than ½ of symptomatic patients with IC have depression. These patients, in turn, report that the stress becomes an exacerbating factor. Neuropathic causes:(Baillie. N. 2003) • This theory proposes that IC is not primarily a disease of the bladder, but of the nervous system.
It has also been suggested that nerve root compression or irritation at the lumber level of the spine can cause IC. Lower back problems need to be taken seriously in people with IC.
Anti-proliferative factor (APF): (Bone, K. 2004) • A break through in IC research has found a peptide – APF – in the urine of IC patients. • It is hypothesised that APF in urine inhibits appropriate bladder epithelial cell regeneration resulting in thinning or denudation of the bladder epithelium. • More studies are ongoing. • Many patients currently being treated for prostatitis who fail to respond to therapy actually may have undiagnosed interstitial cystitis.
Symptoms • Suprapubic pain or pelvic pain • Relieved with small volume voids • Pain recurs with bladder filling • Nocturia • Excessive urinary urgency • Uncomfortable constant urge to void • Not relieved with voiding • Urinary Frequency • More than 8 voids per day • Average: 16 voids per day • Reported as high as 40 voids per day
Symptoms persist over 9 months • Symptoms not due to recent urinary tract infections • Symptoms worse during week before menses • Dyspareunia (difficult or painful intercourse in women) • Gross haematuria (20%) • Incontinence suggests other diagnosis
In the study by Koziol et al of 565 interstitial cystitis patients, urgency and frequency were reported in nearly everyone. With reduced bladder capacity and decreased bladder contractions, subjects urinate as often as every 1-2 hours throughout the day and night, with increasing frequency as the duration of the disease increases. As many as 40% of patients may have one or more episodes of hematuria. • Half of the subjects reported being awakened in the middle of the night because of pain. Two thirds of the subjects reported pelvic pain or pressure, with more than one half reporting pain on intercourse and one third reporting pain for days after intercourse.