Download
1 / 1
10 likes | 101 Vues
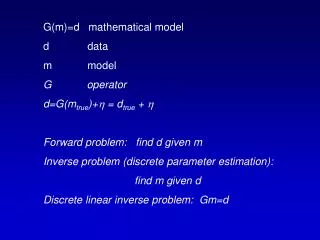
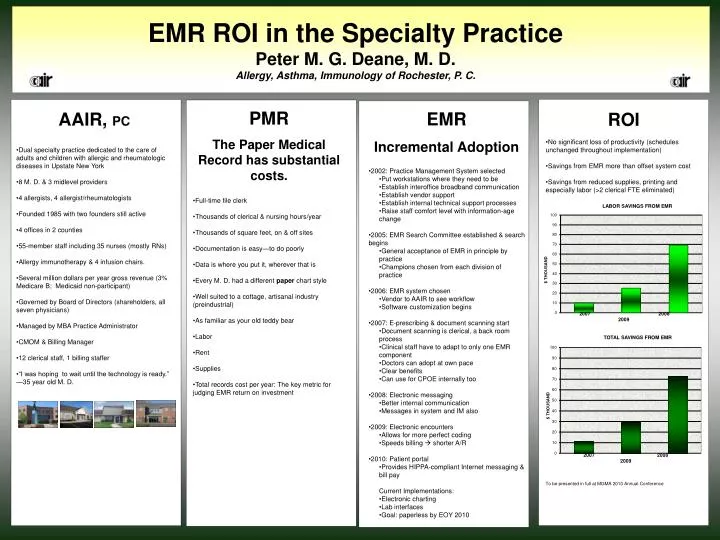
EMR ROI in the Specialty Practice Peter M. G. Deane, M. D. Allergy, Asthma, Immunology of Rochester, P. C. PMR The Paper Medical Record has substantial costs. EMR Incremental Adoption. AAIR, PC. ROI. No significant loss of productivity (schedules unchanged throughout implementation)

E N D
EMR ROI in the Specialty Practice Peter M. G. Deane, M. D. Allergy, Asthma, Immunology of Rochester, P. C. PMR The Paper Medical Record has substantial costs. EMR Incremental Adoption AAIR, PC ROI • No significant loss of productivity (schedules unchanged throughout implementation) • Savings from EMR more than offset system cost • Savings from reduced supplies, printing and especially labor (>2 clerical FTE eliminated) • To be presented in full at MGMA 2010 Annual Conference • Dual specialty practice dedicated to the care of adults and children with allergic and rheumatologic diseases in Upstate New York • 8 M. D. & 3 midlevel providers • 4 allergists, 4 allergist/rheumatologists • Founded 1985 with two founders still active • 4 offices in 2 counties • 55-member staff including 35 nurses (mostly RNs) • Allergy immunotherapy & 4 infusion chairs. • Several million dollars per year gross revenue (3% Medicare B; Medicaid non-participant) • Governed by Board of Directors (shareholders, all seven physicians) • Managed by MBA Practice Administrator • CMOM & Billing Manager • 12 clerical staff, 1 billing staffer • “I was hoping to wait until the technology is ready.” —35 year old M. D. • 2002: Practice Management System selected • Put workstations where they need to be • Establish interoffice broadband communication • Establish vendor support • Establish internal technical support processes • Raise staff comfort level with information-age change • 2005: EMR Search Committee established & search begins • General acceptance of EMR in principle by practice • Champions chosen from each division of practice • 2006: EMR system chosen • Vendor to AAIR to see workflow • Software customization begins • 2007: E-prescribing & document scanning start • Document scanning is clerical, a back room process • Clinical staff have to adapt to only one EMR component • Doctors can adopt at own pace • Clear benefits • Can use for CPOE internally too • 2008: Electronic messaging • Better internal communication • Messages in system and IM also • 2009: Electronic encounters • Allows for more perfect coding • Speeds billing shorter A/R • 2010: Patient portal • Provides HIPPA-compliant Internet messaging & bill pay • Current Implementations: • Electronic charting • Lab interfaces • Goal: paperless by EOY 2010 • Full-time file clerk • Thousands of clerical & nursing hours/year • Thousands of square feet, on & off sites • Documentation is easy—to do poorly • Data is where you put it, wherever that is • Every M. D. had a different paper chart style • Well suited to a cottage, artisanal industry (preindustrial) • As familiar as your old teddy bear • Labor • Rent • Supplies • Total records costper year: The key metric for judging EMR return on investment