Insights into Diabetes Genetics: The Role of Genotype and Environment in T2D Risk
This study explores the complex interplay between genetic factors and environmental influences on type 2 diabetes (T2D) risk through various lenses, including monogenic, syndromic, and multifactorial diabetes. It highlights the findings from HugeNET (Venezia) involving genome-wide association studies and the significance of maternal and paternal genotypes in the risk of T2D across different life stages. Furthermore, the research addresses the challenges of phenotypic variability, heterogeneity in statistical power, and the need for improved methodologies in diabetes genetics.

Insights into Diabetes Genetics: The Role of Genotype and Environment in T2D Risk
E N D
Presentation Transcript
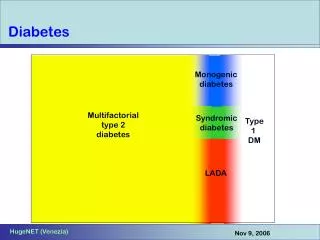
Monogenic diabetes Multifactorial type 2 diabetes Syndromic diabetes Type 1 DM LADA Diabetes HugeNET (Venezia)
environments maternal genotype childhood prenatal adult postnatal risk of T2D individual genotype paternal genotype Genes and environment • familial clustering • twin studies • adoption studies • migration studies • admixture studies • gene discovery • secular trends • migration studies • twin studies • transgenerational effects • intervention studies Environment Genes HugeNET (Venezia)
Activity in the field • ~(3)000 association studies in T2D • Vast majority are small (n=hundreds) case-control studies vulnerable to the usual litany of errors, biases, problems • Growing number (~50) of large (>5000 samples) studies from limited number (4) of groups which have examined ~30 genes (NB many of these in more than one large study); all European eg UK 4000 cases & controls; France 3000; DK 2500; Broad/Lund 5000 • Genome wide association studies underway in ~8000 case-control pairs (by several groups) • Most studies use case-control design….in a few centres these are nested from within larger cohorts (but generally small n) HugeNET (Venezia)
Three steps to failure…. P (no true association given positive finding) Wacholder S et al, JNCI, 2004 HugeNET (Venezia)
Some issues • Cases: T2D = diagnosis of exclusion; no clear basis for subdividing cases into more homogeneous groups; some use population base, others selected for FH+ or early onset • Controls:some use population controls (modest classification bias), others “hypernormal” controls. Should not be a major issue for power or effect size estimation; • Other phenotypes: -- continuous: glucose, HbA1c-- intermediate: beta-cell function, insulin sensitivity-- related: BMI, WHR, lipid measures • Phenotypic accuracy: variable, mostly good • Genotyping accuracy: variable, (historically = poor) • Statistical prowess: variable HugeNET (Venezia)
HNF1A PNDM otherMODY TNDM Other rare syndromes Atlas of diabetes susceptibility Effect size few if any genes up here Large Beyond the scope of genetics! Allele frequency Small Common Rare HugeNET (Venezia)
PPARG Pro12Ala and T2D Altshuler et al, NG, 2000 1.25 relative risk 85% susceptibility allele frequency ~25% attributable risk HugeNET (Venezia)
Kir6.2 (KCNJ11) E23K 1.16 relative risk 40% susceptibility allele frequency ~10% attributable risk Gloyn et al, Diabetes 2003 HugeNET (Venezia)
TCF7L2 Grant, Nat Genetics, March 2006 HugeNET (Venezia)
TCF7L2 associations Grant, Nat Genetics, March 2006 HugeNET (Venezia)
Case control data – relative risks * rs7903146: GRR for comparison of heterozygote and rare homozygote, 1.41 (95% CI, 1.15-1.72) P=8.6x10-4 HugeNET (Venezia)
More TCF7L2 Florez et al, 2006 HugeNET (Venezia)
Tier 1 – definites AUC=58% 2500 T2D, 3500 controls – UK Weedon et al, PLOS Med 2006 HugeNET (Venezia)
Reliability and heterogeneity • For “real” results, relatively little heterogeneity of effect size (I know this is a circular argument…) • Little evidence of GGI or GEI (but then again, how would we know?) • Based on “proven” examples, much harder to find associations with the intermediate traits than with end-phenotypes (presumably because we measure the former so badly) HugeNET (Venezia)
Tier 1: the possibles HugeNET (Venezia)
LMNA • Lamin A/C • Nuclear membrane protein • Associated with diverse disease – laminopathies • Rare mutations familial partial lipodystrophy • ? Association with T2D • Maps to chr 1q: replicated linkage • H556H associations with metabolic syndrome • Monogenic multifactorial: another example? HugeNET (Venezia)
UK study + 2817 1q samples OR 1.07 (0.99-1.15), p=0.08 + other published data OR 1.08 (1.01-1.16), p=0.04 + unpublished dataOR 1.10 (1.04-1.16), p=0.001 Owen KR et al, in press HugeNET (Venezia)
Tier 1: the unlikely ones HugeNET (Venezia)
AXOLOTL consortium • UK • Denmark • Sweden • Cambridge, Mass • KCNJ11, PPARG, CAPN10 • 15k samples • Is there more to PPARG than P12A? Going beyond the association HugeNET (Venezia)
mt3243 LMNA Atlas of diabetes susceptibility Effect size HNF1A PNDM otherMODY few if any genes up here Large TNDM Other rare syndromes TCF7L2 PPARG LARS2 HNF1A KCNJ11 CAPN10 ENPP1 ACDC HNF4A Beyond the scope of genetics! LMNA INS Allele frequency Small Common Rare HugeNET (Venezia)
www.wtccc.com www.wtcc.org.uk Wellcome Trust Case Control Consortium WTCCC: www.wtccc.org.uk HugeNET (Venezia)
To be finalised Affymetrix 500k 2000 malaria 2000 T1D 2000 T2D 2000 Gambiancontrols 2000 RhA 2000 TB 3000 UK common controls 2000 CHD “African” diseases 15k Infinium nsSNP 2000Crohns 2000 HT 1000 MS 1000 BrCa 2700 bipolar 1500 UK common controls Main study with national cases/controls 2000 cohort 2000 obese 1000 thyroid 1000Ank S Obesity case-cohort (Norfolk EPIC) nsSNP experiment 15k Infinium WTCCC HugeNET (Venezia)
WTCCC: controls Nationally representative Unselected for T2D Other forms of diabetes “excluded” Enriched for early onset, FH+ 2000 T1D 2000 T2D 2000 T2D 2000 RhA 3000 UK common controls 2000 CHD 3000 UK common controls 2000Crohns 2000 HT 2700 bipolar 1500 UK blood donor controls 1500Birth Cohort 1958 Main study with national cases/controls Nationally representative Unselected for disease phenotype Common controls Middle-aged – minimise survivor bias Phenotypes++ for 58BC DATA RELEASE…. HugeNET (Venezia)
1000ccp WTCCC 6200ccp PPARG P12A 2000 ~10 KCNJ11 E23K 10-100 3000 TCF7L2 10-100 Gene X MAF 0.15; GRR 1.2; PAR 10% 40000 1400 Even a billion genotypes is not enough Number of positives null alternate:perfect data alternate:real data Uncorrected P HugeNET (Venezia)
Combining data HugeNET (Venezia)
“IGWANA” consortium • Integrated Genome Wide Association ANAlysis in Type 2 Diabetes • Collaborative effort to share data from these (and other) scans toallow joint analyses… • to provide rapid replication of “big” signals • to allow more informed selection of SNP subsets for stage 2 genotyping • to allow formal meta-analysis of genome wide data across >6000 case-control pairs • to exchange experience, ensure high quality research • type 2 diabetes case-control studies (initially, at least) • genome wide association scan data (100k chip entry level) • both summary and individual patient data • contact mark.mccarthy@drl.ox.ac.uk; boehnke@umich.edu; altshuler@molbio.mgh.harvard.edu HugeNET (Venezia)
Direct typing (selected signals) epidemiology DGDG Sequencing genetics DGI physiology SNP selection (p<0.001) combinedanalysis Finemapping 2nd stage genotyping Repli cation WTCCC cell biology FUSION clinical diagnostics CNVs pharmacogenetics Phase III Phase IV Phase 0 Phase I Phase II Follow up joint P<10-2 P<10-6 P<0.001 4000 cases 4000 controls 5000 cases 5000 controls 5500 cases 6500 controls 2000 cases 3000 controls >100,000 samples ~30 signals 0% FPRP ~30 signals <10% FPRP ~1500 SNPs >95% FPRP HugeNET (Venezia)
Summary • Usual mess where small studies are concerned: heterogeneity and untraceable error and unfathomable biases suggest that little to be learned from such studies • More consistent picture when large studies are concerned (as consistent as sample size and effect size will allow) and much better “accountability” • GWA studies offer huge opportunities, but the scale of these studies means that replication, validation, extension is more vital than ever HugeNET (Venezia)