THE STAPHYLOCOCCI
THE STAPHYLOCOCCI. II MBBS Dr Ekta Chourasia Microbiology. CASE. Mrs X, a 30 year old female brought to the hospital by her husband Chief complaint: Fever, erythematous maculopapular rashes over her body & is confused History of High grade fever with chills & body malaise since 2 days

THE STAPHYLOCOCCI
E N D
Presentation Transcript
THE STAPHYLOCOCCI II MBBS Dr Ekta Chourasia Microbiology
CASE • Mrs X, a 30 year old female brought to the hospital by her husband • Chief complaint: Fever, erythematous maculopapular rashes over her body & is confused • History of • High grade fever with chills & body malaise since 2 days • Nausea & vomiting • Steady deterioration in her condition over 24 hours • Menstrual history: She is on day 4 of her cycle. Dr Ekta, Microbiology
CASE • O/E – BP: 80/50 mm Hg HR:120 /min Temp: 103 F Buccal mucosa and tongue – congested • PVE – tampon in place, when removed, reveals a red & inflamed vaginal mucosa. • Blood picture – leucocytosis, thrombocytopenia, abnormal liver function tests and elevated urea & creatinine. Dr Ekta, Microbiology
Case – Microbiology laboratory findings • Specimens – vaginal swab, tampon & blood • Microscopy – gram +ve cocci in clusters • Culture – beta hemolytic colonies on BA • Biochemical tests – catalase & coagulase +ve • Blood culture positive Causative agent – Staphylococcus aureus Dr Ekta, Microbiology
Case – Impression? • Diagnosis - Toxic shock syndrome • Diagnostic features: • High fever • Extensive skin rash • Multisystem involvement – GIT, kidneys, liver, CNS, blood • Inflamed vaginal mucosa with tampon • Microbiological findings Dr Ekta, Microbiology
Classification • Family Micrococcaceae • Genus Micrococcus & Staphylococcus • Species S. aureus S. saprophyticus S. epidermidis M. luteus more than 20 species Dr Ekta, Microbiology
Overview • Main group of medically important gram positive cocci along with streptococci • Infections range from severe to fatal conditions • Difficult to treat, especially those acquired in the hospital • Remarkable ability to acquire antibiotic resistance • Ubiquitous - Part of human flora, inanimate objects Dr Ekta, Microbiology
Overview • Many species are medically important • S. aureus – • most virulent species • Most common cause of bacterial infections, food poisoning & toxic shock syndrome • S. epidermidis – important cause of prosthetic implant infections • S. saprophyticus – UTI, especially cystitis in women Dr Ekta, Microbiology
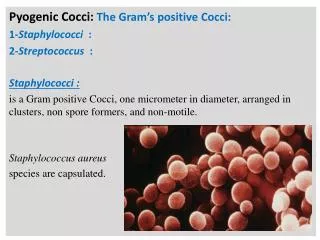
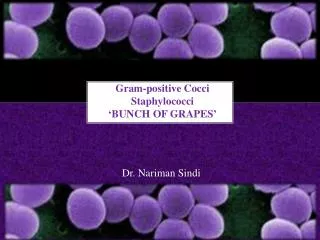
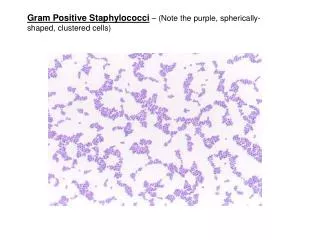
Staphylococci – General features • Gram +ve cocci arranged in grape like cluster • Facultative anaerobes • Produce catalase • Major component of normal flora in humans • Skin • Nose • Mucosal membranes Dr Ekta, Microbiology
Staphylococcus aureus – General features • Coagulase positive • Ferments mannitol • Beta hemolytic colonies on BA • Produces golden yellow pigment • Produces phospahatse • Reduces tellurite producing black colonies • Highly resistant non sporing bacteria • Can grow in the presence of 10 – 15% NaCl. • Resistance to Penicillin Dr Ekta, Microbiology
S. aureus - Epidemiology • Colonise skin, mucosa of anterior nares and vagina • Source of infection – human patients & carriers • About 10-30% of healthy persons carry staphylococci in the nose, about 10% in the perineum and hair. • Vaginal carriage is about 5-10%, which rises during menses. • Modes of transmission – by direct contact or through fomites, by dust or by airborne droplets. • Common cause of postoperative wound infection & other hospital cross infections – multidrug resistant strains. Dr Ekta, Microbiology
Staphylococcus aureus • Diseases produced by S. aureus can be due to • Infection– cocci gain access to damaged skin, mucosa or tissue, colonise at the site, multiply & cause damage • Intoxication – bacterial toxins produced either in the host or preformed invitro • Combination of infection & intoxication. Dr Ekta, Microbiology
Virulence Factors • The virulence of S. aureus depends on a number of factors. These can be: • Cell associated polymers and surface proteins, • Enzymes & • Toxins – cytolytic & superantigen exotoxins Dr Ekta, Microbiology
1. Cell associated polymers & surface proteins • Teichoic acid:- promotes colonization of host tissues • Capsule (slime layer):- inhibits phagocytosis • Protein A:- major component of cell wall, has many biological properties: • Antiphagocytic • Anticomplementary • Binds to the Fc part of IgG • Role in coagglutination – for streptococcal grouping & gonococcal typing Dr Ekta, Microbiology
1. Cell associated polymers & surface proteins • Clumping factor – • a surface protein • Also called “Bound Coagulase” • Responsible for “slide coagulase test” – routinely used for the presumptive identification of S. aureus strains • Saline suspension of S. aureus + drop of human plasma – clumping of cocci • Fibronectin binding protein (FnBP) – binding to mucosa & tissue Dr Ekta, Microbiology
2. Enzymes • Coagulase– • Clotting of human or rabbit plasma in the presence of ‘coagulase reacting factor’ (CRF) • Binds to prothrombin in the plasma & results in the conversion of fibrinogen to fibrin • Responsible for “tube coagulase test” – standard criterion for the identification of S. aureus • Eight types have been identified. • Most human strains form coagulase type A. • No evidence that it is a virulence factor Dr Ekta, Microbiology
2. Enzymes • Staphylokinase (Fibrinolysin) – lysis fibrin clots, spread of infection • Hyaluronidase – breaks down the connective tissue, initition & spread of infection • Lipase – infection of skin & subcutaneous tissue • Nuclease– degrades DNA • Catalase – • enhance their survival in phagocytes by inactivating toxic H2O2 & free radicals released after the ingestion of staphylococci. Dr Ekta, Microbiology
3. Toxins • Cytolytic exotoxins: hemolysins (alpha, beta, gamma & delta), leucocidins - membrane active substances • Alpha hemolysin • Most potent membrane-damaging toxin • Toxin subunits create a central pore through which cellular contents leak • Septic shock • Beta hemolysin • Sphingomyelinase - damages membranes rich in this lipid • Leucocidin • important factor in necrotizing skin infections.) Dr Ekta, Microbiology
3. Toxins • Superantigen exotoxins • Enterotoxin: Eight antigenic types - A, B, C 1 to 3, D, E and H, causes food poisoning • Toxic shock syndrome toxin (TSST) • Exfoliatin (epidermolytic toxin) Dr Ekta, Microbiology
Pathogenicity (staphylococcal diseases) Dr Ekta, Microbiology
Pathogenicity • Skin & soft tissue infections • Localized skin infection - Folliculitis, furuncle (boil), carbuncle, abscess (particularly in breast), wound infection (surgical, traumatic), impetigo • Deep, localized infections – Osteomyelitis (S. aureus is the most common cause), arthritis (septic arthritis in children) • Respiratory tract infections • bronchopneumonia, tonsillitis, pharyngitis, sinusitis, lung abscess, empyema Dr Ekta, Microbiology
Pathogenicity • CNS infections – abscess, meningitis, intracranial thrombophlebitis • Endovascular – bacteremia, septicemia, pyemia, endocarditis • Urinary tract infectionoften in association with local instrumentation, implants or diabetes • Nosocomial infections – wound infection, catheter associated bacteremia. Dr Ekta, Microbiology
Pathogenicity • Staphylococcal food poisoning • Occurs 1 to 6 hrs after consumption of food contaminated with preformed toxins (enterotoxins – very fast acting) • Nausea, vomiting, abdominal cramps & diarrhoea • Self limiting condition, 1 to 3 days • Toxins are resistant to heat, resistant to cooking • Highest risk of contamination: sliced meat, puddings, pastries, sandwiches, milk & cheese • Source of infection – food handler • Type A enterotoxin is responsible for most cases Dr Ekta, Microbiology
Pathogenicity • Toxic shock syndrome • Caused by TSST-1 (formerly known as Enterotoxin F): responsible for 75% of TSS, including all menstrual (tampon related TSS) cases • Enterotoxins B and C cause 50% of non-menstrual cases of TSS • Mostly in females however cases have been reported in males as well (e.g. surgical site infection) • Fatal multisystem disease Dr Ekta, Microbiology
Tampon - Associated with outbreak of toxic shock syndrome. Dr Ekta, Microbiology
Signs And Symptoms :TSS • Prodromal period of 2-3 days • High grade fever and/or chills • Nausea and/or vomiting • Profuse watery diarrhea with abdominal pain • Mucosal hyperemia (vaginitis, conjunctivitis) & erythematous rash which desquamates in 1-2 weeks • Myalgias and/or arthralgias • Headache • Confusion (more common with staphylococcal TSS than with streptococcal TSS) Dr Ekta, Microbiology
Skin Rash: starts from trunk and then spreads to the periphery (legs & arm) Dr Ekta, Microbiology
The Centers for Disease Control and Prevention (CDC) criteria for the diagnosis of staphylococcal TSS • Fever, hypotension, and rash • Involvement of 3 or more organ systems • Absence of serologic evidence of Rocky Mountain spotted fever, leptospirosis, measles, hepatitis B, antinuclear antibody, positive Venereal Disease Research Laboratory (VDRL) test results, and antibodies at Monospot testing Dr Ekta, Microbiology
Pathogenicity • Staphylococcal scalded skin syndrome (SSSS) • Exfoliative skin disease – outer layer of epidermis gets separated from the underlying tissues • Cause – exfoliative toxin that damages desmosomes • Severe form of SSSS is • “Ritter’s Disease” in newborns and • Toxicepidermal necrolysis in older patients • Milder forms are • Pemphigus neonatorum • Bullous impetigo Dr Ekta, Microbiology
SSSS • Signs And Symptoms: • Fever • Generalized erythema • skin slips off with gentle pressure leaving wet red areas (Nikolsky sign) • exfoliation or desquamation • painful skin • Treatment: • Fluid rehydration • Topical wound care: saline AND topical antibiotic ointment Dr Ekta, Microbiology
Prognosis: SSS • Healing begins in about 10 days following treatment. • A full recovery is expected. • Possible Complications • septicemia • dehydration or electrolyte imbalance • poor temperature control (in young infants) • cellulitis • The disorder may not be preventable; Prompt treatment Dr Ekta, Microbiology
Laboratory diagnosis • Specimen – depends on type of lesion • Pus - Suppurative lesion • Sputum – respiratory tract infection • Feces & remains of food – food poisoning • Blood – septicemia • Nasal swab – detection of carriers • Microscopy • Gram stain – gram +ve cocci in clusters Dr Ekta, Microbiology
Laboratory diagnosis • Culture – specimens are plated on • NA - golden yellow colony • BA – hemolytic colonies • Selective media – Ludlam’s media, Mannitol salt agar (MSA) MSA Dr Ekta, Microbiology
Laboratory diagnosis • Biochemical tests • Catalase test – using 3% H2O2 :all Staphylococci are catalase positive, gives effervescence Dr Ekta, Microbiology
Laboratory diagnosis • Biochemical tests • Coagulase test – S. aureus is coagulase +ve • Done by two methods • Slide coagulase test – detects bound coagulase (clumping factor) • Tube coagulase test – detects free coagulase • Bacteriophage typing - for epidemiological purposes Dr Ekta, Microbiology
Staphylococcus aureus Coagulase POS Coagulase NEG Dr Ekta, Microbiology
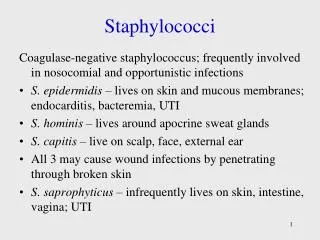
Coagulase-negative Staphylococci(CONS) • S. epidermidis;75% of clinical isolates • S. saprophyticus • S. haemolyticus • S. hominis • S. capitis Dr Ekta, Microbiology
General features of CONS • Important agents of nosocomial infections • Associated with increased use of implants such as CSF shunts, IV lines, cardiac valves, pacemakers, artificial joints, urinary catheters • Morphologically similar to S. aureus, however they form white colonies, and are coagulase negative. Dr Ekta, Microbiology
S. epidermidis Dr Ekta, Microbiology
Disease Caused By Coagulase-negative Staphylococci • Prosthetic valve endocarditis • Meningitis • Peritonitis • UTI in pregnant women (S. saprophyticus) • Treatment is with Vancomycin, if not resistant. S. saprophyticus responds to trimethoprim or to quinolones. Dr Ekta, Microbiology
Differences between the major species of Staphylococci Dr Ekta, Microbiology
Treatment • Drain infected area • Deep/metastatic infections • semi-synthetic penicllins • cephalosporins • erythromycin • clindamycin • Endocarditis • semi-synthetic penicillin + an aminoglycoside • Life threatening staphylococcal infections, Vancomycin is the drug of choice • However, the appropriate antibiotic should be chosen based on AST. Dr Ekta, Microbiology
Drug Resistance in Staphylococci • First developed resistance against Penicillin • Resistance to penicillin can be due to: • Mutation in chromosomal genes followed by selection of resistant strains • Acquisition of resistance genes as extrachromosomal plasmids, transducing particles, transposons, or other types of DNA inserts. • Production of penicillinases • Changes in bacterial surface receptors • Development of tolerance Dr Ekta, Microbiology
Drug Resistance in Staphylococci • To combat resistance due to penicillinase, Methicillin was developed & now methicillin resistant strains have evolved due to • Chromosomal acquisition of gene coding for a modified PBP • Plasmid borne resistance to erythromycin, tetracyclines, aminoglycosides and almost all clinically useful antibiotics Dr Ekta, Microbiology
MRSA(Methicillin resistant S. aureus) • occur in otherwise healthy people who have not been recently (within the past year) hospitalized • had a medical procedure (such as dialysis, surgery, catheters) • community-associated (CA)-MRSA infections skin infections: abscesses, boils, and other pus-filled lesions Dr Ekta, Microbiology
MRSA Reservoirs • In hospitals, the most important reservoirs of MRSA are infected or colonized patients • HOSPITAL PERSONNEL: commonly identified as a link for transmission between colonized or infected patients. Dr Ekta, Microbiology
Mode Of Transmission: MRSA • via hands (especially health care workers') which may get contaminated by contact with • colonized or infected patients • colonized or infected body sites of the personnel themselves, • devices, items, or environmental surfaces contaminated with body fluids containing MRSA. Dr Ekta, Microbiology
Treatment: MRSA • Glycopeptides • Vancomycin • Teicoplanin Dr Ekta, Microbiology
VRSA • 1996, MRSA strains with decreased susceptibility to vancomycin • VISA: if the MIC for vancomycin is 4-8µg/ml, • VRSA :MIC is >16µg/ml. Dr Ekta, Microbiology
VISA, VRSA • several underlying health conditions (such as diabetes and kidney disease) • previous infections with methicillin-resistant Staphylococcus aureus (MRSA) • intravenous [IV] catheters • recent hospitalizations • recent exposure to vancomycin and other antimicrobial agents. Dr Ekta, Microbiology