Download
1 / 30
300 likes | 373 Vues
Screening for Obstructive Sleep Apnea (OSA) & Surgical Risk: Development of a New Process. Kelly Pick, MSN RN-BC NPD Clinical Educator: Patient and Community Education. Objectives. At the end of this presentation, the learner will be able to:

E N D
Screening for Obstructive Sleep Apnea (OSA) & Surgical Risk: Development of a New Process Kelly Pick, MSN RN-BC NPD Clinical Educator: Patient and Community Education
Objectives At the end of this presentation, the learner will be able to: • Analyze the process of developing and implementing a multidisciplinary and multi‐site team approach to prevention of OSA‐related post‐surgical complications. • Explain the meaning of STOP‐BANG and the Epworth Sleepiness scale and their use in screening for OSA. • Evaluate various patient education materials used for teaching patients/Key Learners about OSA and pre‐surgical screening.
What is Obstructive Sleep Apnea? Obstructed Airway Normal Airway
Steps in the Process • Identify the problem • Gather info • Gather team • Kaizen event • Break up into teams • Develop materials • Work out the bugs • Go Live • Staff Education • Work out more bugs • Constant re-evaluation
Original plan: Ortho surgeries with certain MD groups Now: All surgeries (all MDs) (including OB) Scope Creep
OBSTRUCTIVE SLEEP APNEA in the Hospital Setting“Why Patient Safety Professionals need to be concerned about OSA and what to do about it”March 2011 – WSHA Safe Table (Excerpts) Stephanie Jackson MD, FHM System Patient Safety Officer - PeaceHealth
Obstructive Sleep Apnea • Prevalence • 2-10% in women • 4-25% in men • > 80% of patients have not been diagnosed • Increased risk: • Age: changes to connective tissue relax the tissues in the back of the throat • Obesity: 70% of bariatric patients • Hypertension
OSA in the Hospital Environment • 2.5x increased risk for post op complications • Opiates, sedatives, and anesthetics decrease brain’s ability to respond to rising CO2 levels • Myth : Obese pts need higher doses of drugs -> can have catastrophic consequences
Opiates, Benzos and OSA : The Perfect Storm • Anesthetic agents, sedatives, and opiates • Muscle tone • Sleep arousal • Ventilation • Response to carbon dioxide • Lingering effects
Why are we doing this now? • American Society of Anesthesiologists (ASA) guidelines on Peri-operative OSA management • Obesity Epidemic • Litigation environment on OSA • Serious adverse events
The Wake up CALL • Known Sleep apnea in post-elective Knee Replacement • Issues with pain control • Not using CPAP • Not on central monitoring • Nurse gave some dilaudid and a benzodiazapine • Heard him snoring loudly outside the room • Came in 15 minutes later to check and patient had arrested • Resuscitated him, but he had irreversible brain damage and later died
Another Case: • Combination of opiates, benzodiazepines, ETOH, and unrecognized sleep apnea • During an MRI- young morbidly obese man was snoring loudly • Stopped breathing • Coded and died
A More Recent Case: • Recent foot amputation for a diabetic • Protocol was ordered but the orders were not taken off • Respiratory arrest • Died
RN Web Lesson (Excerpts) Assigned to all RNs at PHSW
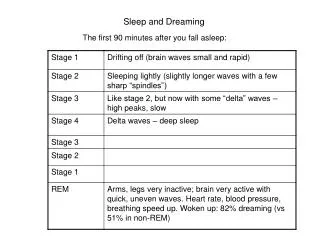
Obstructive Sleep Apnea (OSA) • Mechanics of breathing • Two factors that affect our breathing: • oxygen (hypoxemia) • carbon dioxide (hypercarbia)
Pathophysiology of an apneic episode Obstructive Sleep Apnea (OSA) Airway obstructed breathing oxygen, CO2 Brain signals body
Obstructive Sleep Apnea (OSA) • What is the health concern (other than snoring?): • Sleep cycle • Hypertension • Heart Attack and Stroke • Insulin Resistance (Hypoxic stress of sleep apnea) • Sudden Death Events • Additionally in the post-op patient receiving sedation and pain control: • Respiratory depression acute hypoxia • CO2 acidosis and cell death
Obstructive Sleep Apnea (OSA) • How is OSA diagnosed? • Gold standard: polysomnography (sleep study) • STOP-BANG Screen • Referral for sleep study prior to elective surgery • And how is it treated? • CPAP or BIPAP
Obstructive Sleep Apnea (OSA) • Perioperative Care of the OSA or Suspected OSA patient: • Frequent assessment: sedation level and pain control • Pulse oximetry • Capnography • Supplemental O2: 88-94% (or per provider orders). Avoid O2 sats > 94% • CPAP from home (Known OSA) • RT consult (Suspected OSA) for BIPAP
STOP-BANG S: Snoring T: Tired O: Observed apnea P: High blood Pressure B: BMI > 35 A: Age > 50 N: Neck size- >17” male; >16” female G: Gender- Male
Inclusion Criteria • No set criteria in the literature (ranged from 3-5) • Team agreed on >4 automatically included • If <3, check co-morbidities • Recurrent PACU respiratory event or respiratory event in OR • BMI >40 • BMI >35 And Hx of Pulmonary Hypertension • BMI >35 And serum bicarb >27 [hypoventilation syndrome] • May use CO2 from past 6 months • If no results in last 6 months, order CO2 if BMI between35 and 40
Epworth Sleepiness Scale http://epworthsleepinessscale.com/
ESS :What’s Normal? Normal: 0-10 Mean: 4.6
Other collateral Desk reference notebooks Orders (Electronic and Downtime) CNA Education Provider Education Procedures Workflow Staff Education Posters Patient Education Materials Pre-op Checklist ISBARQs Policies Standards of Care Electronic Admission History with STOP-BANG
Lessons Learned • One big lesson is that it would be great to have all the main players from the beginning of a project so that things move more smoothly. It's hard when you start a project and then half way through, you realize other key players need to be there. • Policies and procedures put in place without the input of those it affects seem destined to fail. Besides, everyone appreciates having some say. • We should have seen the issues surrounding D/C with CPAP before go live. • It took several meetings together in the beginning for the Project Team to understand really what each member needed so that they each could get their parts done. • By the nature of the process, various individuals' roles and responsibilitieschanged as the project evolved. • I feel that some other team members had to step in and finish other team members commitments to get the project rolling.