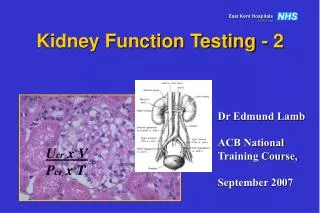
Kidney Function Testing
Kidney Function Testing. MALIK ALQUB MD. Ph. D. MAJOR CAUSES OF KIDNEY DISEASE .

Kidney Function Testing
E N D
Presentation Transcript
Kidney Function Testing MALIK ALQUB MD. Ph. D.
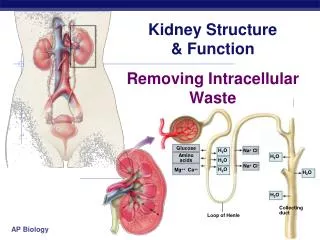
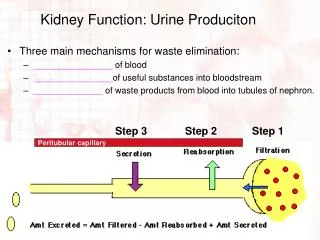
MAJOR CAUSES OF KIDNEY DISEASE • The causes of acute or chronic kidney disease are traditionally classified by that portion of the renal anatomy most affected by the disorder. Renal function is based upon four sequential steps, which are isolated to specific areas of the kidney or surrounding structures: • First, blood from the renal arteries and their subdivisions is delivered to the glomeruli. • The glomeruli form an ultrafiltrate, nearly free of protein and blood elements, which subsequently flows into the renal tubules. • The tubules reabsorb and secrete solute and/or water from the ultrafiltrate. • The final tubular fluid, the urine, leaves the kidney, draining sequentially into the renal pelvis, ureter, and bladder, from which it is excreted through the urethra.
Prerenal disease • The two major causes of reduced renal perfusion are volume depletion and/or relative hypotension. This may result from true hypoperfusion due to bleeding, gastrointestinal, urinary, or cutaneous losses, or to effective volume depletion in heart failure, shock, or cirrhosis. • Prerenal disease is most commonly associated with an acute time course. However, among patients with chronic kidney disease, the addition of a prerenal process may result in acute renal dysfunction
Glomerular disease • There are numerous idiopathic and secondary (due to neoplasia, autoimmunity, drugs, genetic abnormalities, and infections) disorders that produce glomerular disease. Two general patterns (with considerable overlap in some diseases) are seen: • A nephritic pattern, which is associated with inflammation on histologic examination and produces an active urine sediment with red cells, white cells, granular and often red cell and other cellular casts, and a variable degree of proteinuria. • A nephrotic pattern, which is not associated with inflammation on histologic examination and is associated with proteinuria, often in the nephrotic range, and an inactive urine sediment with few cells or casts.
Tubular and interstitial disease • As with vascular disease, the tubular and interstitial diseases affecting the kidney can be divided into those that produce acute and chronic disease: Hereditary, systemic, toxic, and drug-induced causes predominate. • The most common acute tubulointerstitial disorders are acute tubular necrosis, which typically occurs in hospitalized patients. • The major chronic tubulointerstitial disorders are polycystic kidney disease
Obstructive uropathy • Obstruction to the flow of urine can occur anywhere from the renal pelvis to the urethra. The development of renal insufficiency in patients without intrinsic renal disease requires bilateral obstruction (or unilateral obstruction with a single functioning kidney) and is most commonly due to prostatic disease (hyperplasia or cancer) or metastatic cancer. The time course can be acute or chronic
The nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular filtration barrier. It is classically characterized by four clinical features, but the first two are used diagnostically because the last two may not be seen in all patients: • Nephrotic range proteinuria — Urinary protein excretion greater than 50 mg/kg per day • Hypoalbuminemia — Serum albumin concentration less than 3 g/dL (30 g/L) • Edema • Hyperlipidemia
Pathophysiology of SN Glomerulus damage PROTEINURIA
Pathophysiology of SN • Proteinuria • Increased filtration of macromolecules across the glomerular capillary wall • Commonly due to abnormalities in podocytes • Increased loss of: • Albumin • Clotting inhibitors • Transferrin • Hormone binding proteins (e.g., Vit D binding protein)
Pathophysiology of SN • Hypoalbuminemia • Unclear why hepatic synthesis can not compensate sufficiently • Edema • Marked hypoalbuminemia leading to movement of fluid into the interstitial space by decreasing plasma oncotic pressure • Primary renal sodium retention in collecting tubules
Clinical Presentation • Generalized Odema • -The predominant feature • -The face, particularly the • periorbital area, is swollen • in the morning& lower extremities • and genital area later in the day • -In advanced disease: the whole boday(anasarca) • Frothy urine and urine dipstick • proteinuria value of +++ • Symptoms & signs for secondary cause if present
Etiology Primary (idiopathic): • Minimal change disease Most common cause in children • Membranous Nephropathy Most common cause in Adults • Focal Segmental Glomerulosclerosis • MembranoProliferative Glomerulonephritis
Etiology Secondary to: • DM(the leading cause of secondary nephrotic syndrome) • SLE • Amyloidosis • Infections: • Hepatitis B and C, HIV, syphilis, post-streptococcal • Malignancy: • multiple myloma , Hodgkin lymphoma, solid tumor • Drugs • (NSAIDs, gold, penicillamine ,heavy metals etc).
1st Goal: To confirm the clinical diagnosis • 24-hour urine collection> 50 mg/kg per DAY (nephrotic-range proteinuria) 2nd Goal: to seek a possible cause • The history and physical examinationSystemic disease • Serologic studies(ANA), complement, hepatitis B and hepatitis C serologies and the measurement of cryoglobulins ,serum or urine protein electrophoresis. ; LFT’s; ASOT; C3/C4; Varicella titres • Renal biopsy required to establish the diagnosis in most of times.
3rdGoal: To assess renal function BUN, creatinine, creatininclearnce.Na, K,bicarbonates,chloride, A urinary sodium concentration can be helpful in those at risk of hypovolaemia. 4th Goal: to identify biochemical disorders related to the nephrotic state. CBC , serum albumin, serum proteins, calcium, Lipid profile, Coagulation tests
Definition of acute renal failure • Acute renal failure (ARF) has traditionally been defined as the abrupt loss of kidney function that results in the retention of urea and other nitrogenous waste products and in the dysregulation of extracellular volume and electrolytes. The loss of kidney function is most easily detected by measurement of the serum creatinine which is used to estimate the glomerular filtration rate (GFR)
Etiology of ARF ARF may be Pre-renal (75%) Renal (20%) Post-renal (5%)
Diagnostic criteria of ARF • The proposed diagnostic criteria for ARF are an abrupt (within 48 hours) absolute increase in the serum creatinine concentration of ≥0.3 mg/dL (26.4 micromol/L) from baseline, a percentage increase in the serum creatinine concentration of ≥50 percent, or oliguria of less than 0.5 mL/kg per hour for more than six hours • normal Cr: • Female 50-90 µmol/L • Male 70-120 µmol/L
The definition of chronic kidney disease • Evidence of structural or functional kidney abnormalities (abnormal urinalysis, imaging studies, or histology) that persist for at least three months, with or without a decreased GFR. The most common manifestation of kidney damage is persistent albuminuria, including microalbuminuria. • OR • Decreased GFR, with or without evidence of kidney damage. GFR < 60 ml/min/1.73m2 for 3 month
Who are at Risk for CKD • Diabetes • Hypertension • Age , Family H/o Kidney Disease • Systemic Infections • Recurrent UTI • Urinary Stone Disease • Loss of Renal mass • Neoplasia of any part • Nephrotoxic Drugs (NSAIDs)
Other Glomerulonephritis 10% 13% Diabetes Hypertension 50.1% 27% The Two Most Common Causes of CKD Primary Diagnosis for Patients Who Start on Dialysis
Treatment of End Stage Renal Failure • Hemodialysis • Uses a mechanized filter to remove impurities from the blood system • Essentially replaces kidney with a machine • Dialysis usually occurs a couple times per week.
Calculation of the creatinine clearance • GFR = [UCr x V]/SCr • SCr = 1.2 mg/dL (106 µmol/L)UCr = 100 mg/dL (8800 µmol/L) V = 1.2 L/day • Then, CCr = [100 mg/dL x 1.2 L/day] / 1.2mg/dL = 100 L/day
This value has to be multiplied by 1000 to convert into mL and then divided by 1440 (the number of minutes in a day) to convert into units of mL/min: CCr = [100 L/day x 1000 ml/L] /1440 min/day = 70 mL/min
creatinine clearance to body surface area (BSA) • A patient's creatinine clearance should ideally be adjusted to body surface area (BSA) when comparing to normal values. • As an example, a creatinine clearance of 70 mL/min in a small woman with a weight and height of 50 kg and 160 cm, who has a BSA of 1.5 kg/m2, is corrected to a body surface area of 1.73 m2 as follows: • CCr x 1.73/BSA = [70 mL/min x 1.73] / 1.5 = 80 mL/min per 1.73 m2
In turn, for a large person with a body surface area of 1.9 kg/m2, the adjusted CCl would be 64 mL/min per 1.73 m2. • The normal value for the creatinine clearance is 95 ± 20 mL/min in women and 120 ± 25 mL/min in men.
Cockcroft & Gault Formula • Cockcroft & Gault Formula • CC = k[(140-Age) x weight(Kg))] / serum Creatinine (µmol/L) • k = 1.224 for males & 1.04 for females • Modifications required for children & obese subjects • Can be modified to use Surface area
GFR = [UCr x V]/SCr • SCr = 1.2 mg/dL (106 µmol/L)weight=60 age = 34 years • CCr(mL/min) = k[(140-Age) x weight(Kg))] / serum Creatinine (µmol/L) • CCr(mL/min)= ((140 – 34)*60)/106 = 60 ml/min
Review questions • 1-Intrarenal acute renal failure can be due to a- dehydration and increased cardiac output b- calculi in the ureters and hypovolimic shock c- antibiotics and radiocontrst dye administration d-obstructed Foley catheter and prostate hypertrophy (c)
3- Decreased erythropoietin production in renal failure results in • a- decreased RBC survival • b-impaired white blood cell function • c- decreased red blood cell production • d-an inability of platelets to function properly (c)
Clinical Case #1 • Ali is a 15 year old male who presented with URI (upper Respiratory Infection) symptoms, then headache, vomiting, abdominal pain, knee pain, edema, and a purpuric rash on his legs. He had not voided for 24 hours. • What is the diagnosis? • ARF? What the lab. Investigations that confirm the diagnosis?
Physical exam and labs • BP was 152/94. Heart and lung exams were normal. Indicate • hypertension • A urinalysis revealed hematuria and proteinuria. BUN and Creatinine were 76 and 8.0. Albumin was 3.1 indicate • ARF
Back to Ali (Clinical case #1) • K+ 6.5, • Bicarb. 14 • Calcium 5.8, Phosphorus 9.3 • Hematocrit 30.3%, Platelets 280K • Interpret this results. • low bicarb. = Metabolic Acidosis
Clinical Case #2 • Samira. is a 10 year-old with acute lymphocytic leukemia receiving chemotherapy • Has fever, neutropenia and thrombocytopenia • UOP (Urinary output) is 1.2 cc/kg/hour • On clinical exam she has very moist mucus membranes • BUN and Creatinine are 110 and 0.7. • Albumin is 3.5
Assessment of clinical case #2 • Is she in renal failure? • Creatinine is normal, so NO! • Why is BUN so high?
Calcium and phosphate metabolism in renal failure • Renal failure is characterized by a decrease in the functioning renal mass and, therefore, in the total glomerular filtration rate (GFR). • there is a reduction in the filtered phosphate consequently in phosphate excretion. • If intake remains constant, the net effect will be phosphate retention and a small increase in the plasma phosphate concentration. • This mild phosphate retention is related to the development of secondary hyperparathyroidism. • Then marked increase in circulating PTH levels
Calcium and phosphate metabolism in renal failure • In kidney failure there is decreased renal excretion of phosphate and diminished production of calcitriol (1,25-dihydroxyvitamin D) • Calcitriolincreases serum calcium levels • The increased phosphate and reduced calcium, feedback and lead to secondary hyperparathyroidism, metabolic bone disease, soft tissue calcifications and other metabolic abnormalities
Hyperparathyroidism • Increase PTH is hallmark of secondary hyperparathyroidism • The major factors leading to it’s increase are; • (uncertain) Decreased serum calcium • Increased serum phosphorous
4 or more small glands on the posterior surface of the thyroid gland.
Bone Disease in CKD • Renal Osteodystrophy
Anemia in CKD • Definition • Hgb • <12 (females) • <13.5 (males)
Anemia in CKD • Frequency of pts with anemia (Hgb <12 in females and <13 in males)