Download
1 / 49
530 likes | 850 Vues
Measurement of Kidney Function. Sophia Arunselvan MD. The basic unit of the kidney is the nephron, with each kidney in humans containing approximately 1.0 to 1.3 million nephrons. CLINICAL MEASUREMENT OF RENAL FUNCTION IS USUALLY VERY CLUMSY. EXCRETION BY NEPHRON.

E N D
Measurement of Kidney Function Sophia Arunselvan MD
The basic unit of the kidney is the nephron, with each kidney in humans containing approximately 1.0 to 1.3 million nephrons
CLINICAL MEASUREMENT OF RENAL FUNCTION IS USUALLY VERY CLUMSY
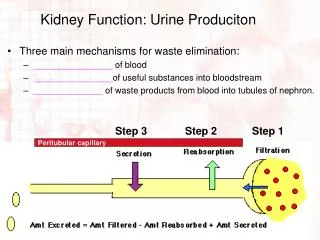
EXCRETION BY NEPHRON • The initial step in the excretory function of the nephron is the formation of an ultrafiltrate of plasma across the glomerulus. • This fluid then passes through the tubules and is modified in two ways: by reabsorption and by secretion. • Reabsorption refers to the removal of a substance from the filtrate • Secretion refers to the addition of a substance to the filtrate. • Reabsorbtion and secreation affect measuring renal function.
Purpose of assessing renal function • Early detection of renal failure for prevention. • Measure disease progression • Prognosis and initiation of treatment • If Therapy is effective • Risk for Cardiovascular disease with renal failure and microalbuminuria
ASSESSMENT OF RENAL FUNCTION • Glomerular filtration rate • Creatinine • Urea • UA
Glomerular filtration rate - GFR • Sum of Filtration rate of all functioning nephrons • GFR=125 ml/mt/1.73m2 = 180 litre/day of plasma filtered a day • Varies widely- age, sex, body size, diet, drugs, pregnancy etc. • Declines with age , increase with pregnancy, 10% lower at midnight
GFR • Used clinically to assess severity of renal failure • Not an exact correlation between the loss of kidney mass and loss of GFR • stable GFR does not necessarily imply stable disease • Normal GFR does not imply normal kidney eg PCKD. • Does not provide info on type/cause of disease
Measurement of GFR • Cannot be Measured directly • Measured as urinary clearance of ideal filtration marker. • Clearance= volume of plasma cleared of a marker by excretion /unit of time
Urinary clearance • Cx = Ux V Px • Urinary clearance measure of GFR if substance filtered but neither secreated or reabsorbed. • If secreated then Cx > GFR • If reabsorbed Cx < GFR • Timed urine collection
Plasma Clearance • Bolus IV exogenous marker • Cx = Equals amount administered / Px over time • Depends on secreation, reabsorbtion and extrarenal elimination.
Ideal Filtration maker • Solute that is freely filtered at the glomerulus • nontoxic • No protein binding • neither secreted nor reabsorbed by the kidney tubules • No extrarenal elimination • Easily measured • cheap • If these criteria are met, the filtered load is equal to the rate of urinary excretion
Exogenous filtration markers • Inulin – Gold standard markers of GFR • Inulin is inert and does not bind to plasma proteins. • It distributes in extracellular fluid, is freely filtered at the glomerulus, and is neither reabsorbed nor secreted by renal tubules • Filtered = excreated
Inulin • short supply • expensive • difficult to assay • Continous IV infusion, various blood samples, foley • Certain situations only- kidney donation, toxic chemotherapy etc
Other Exogenous markers • Iothalamate (IV/SQ) – secreated-overestimate • Iohexol – (IV) –expensive • EDTA (51Cr) – ethylene diamine tetra acetic acid – given IV – 10% lower clearance than inulin • DTPA(99m Tc) – diethylene triamine penta acetic acid – given (IV) - dissociation of Tmc leads to protein binding , underestimation GFR. • chelated to radioisotopes for ease of detection
Endogenous filtration markers • Creatinine • Urea • Cystatin C
Creatinine • Creatinine is a metabolic product of creatine and phosphocreatine, both of which are found almost exclusively in muscle • freely filtered • neither reabsorbed nor metabolized • 10 to 40 percent of urinary creatinine is derived from tubular secretion in the proximal tubule
Serum creatinine concentration is probably the most widely used indirect measure of GFR- Mean serum creatinine values for men and women were 1.13 and 0.93 mg/dL • Convenience and low cost. • Unfortunately, serum creatinine is very insensitive.
Dietary change – meat meal • Dietary supplement • Drugs – trimethoprim, cimetidine. • Amputation • Malnutrition • Muscle wasting • Age – old , low cr • Race eg black vs hispanics/caucasians • Sex
Extrarenal elimination • More Accurate if GFR < 60 ml/mt and steady kidney function • acute kidney injury, for example, the GFR is markedly reduced but there has not yet been time for creatinine to accumulate and, therefore, for the serum creatinine to reflect the degree of renal dysfunction • nephrotic syndrome and sickle cell disease may have a GFR that is substantially lower than what can be estimated from the serum creatinine due to increased secreation
Creatinine clearance • CrCl = 24 hr Ucr x urine volume serum creatinine • Urine collection problems • Overestimates – use cimetidine. • At lower GFR, cr excreated by secreation exceeds filtered amount.
Example — Suppose that the following 24-hour urine results are obtained in a 60 kg woman: SCr = 1.2 mg/dL (106 micromol/L)UCr = 100 mg/dL (8800 micromol/L) V = 1.2 L/day CCr = [100 mg/dL x 1.2 L/day] / 1.2 mg/dL = 100 L/day • To convert this value into units of mL/min, it has to be multiplied by 1000 to convert into mL and then divided by 1440 (the number of minutes in a day): CCr = [100 L/day x 1000 ml/L] /1440 min/day = 70 mL/min • results should ideally be normalized to a body surface area (BSA) of 1.73 m2; As an example, a creatinine clearance of 70 mL/min in a small woman with a weight and height of 50 kg and 160 cm, who has a BSA of 1.5 kg/m2, is normalized to a BSA of 1.73 m2 as follows: CCr x 1.73/BSA = [70 mL/min x 1.73] / 1.5 = 80 mL/min per 1.73 m2 • For a large person with a body surface area of 1.9 kg/m2, the adjusted CCr would be 64 mL/min per 1.73 m2.
Formulae for Estimation of GFR(eGFR) using S.Cr • Cockcroft-Gault equation • Modification of Diet in Renal Disease (MDRD) Study equations • Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation
estimate by Cockcroft-Gault equation (140 - age) x lean bodyweight [kg] crcl (ml/mt) = ————————————Cr [mg/dL] x 72 • For women, the formula requires multiplication by 0.85 to account for smaller muscle mass compared with men • higher weight may mean greater fat mass, and not greater muscle mass. • Not adjusted for body surface area • Measure CrCL • Not precise • Overestimates • Drug dosing guidelines have historically been developed using the Cockcroft-Gault equation to estimate kidney function
MDRD • GFR, in mL/min per 1.73 m2 = 175 x SCr (exp[-1.154]) x Age (exp[-0.203]) x (0.742 if female) x (1.21 if black) • Validated in Dm nephropathy, transplant recipients, AA • Not validated for pregnant, children, elderly> 85.
less accurate in populations with GFR > 60ml/mt – underestimates • Obese-less accurate • overestimate GFR in Japan and some other Asian populations, possibly related to differences in body mass and diet • China showed that the MDRD study equation underestimated GFR
CKD-EPI 141 × min(Cr/κ, 1)α × max(Cr/κ, 1)–1.209 × 0.993Age × 1.018 (if female) × 1.59 (if black) where κ is 0.7 for females and 0.9 for males α is –0.329 for females and –0.411 for males, min indicates the minimum of Cr/κ or 1, and max indicates the maximum of Cr/κ or 1.
The CKD-EPI equation was developed to provide a more accurate estimate of GFR among individuals with normal or only mildly reduced GFR (ie, above 60 mL/min per 1.73 m2 • CKD-EPI equation was as accurate as the MDRD study equation among individuals with estimated GFR less than 60 mL/min per 1.73 m2 and somewhat more accurate in those with higher GFRs • Still limited by imprecision
Plasma urea • Urea was one of the first indicators used to measure GFR. • production is variable and is largely dependent on protein intake • urea is freely filtered at the glomerulus • readily reabsorbed, and the amount of tubular reabsorption is variable
The rate of urea production is not constant, increasing with a high protein diet , protein catabolised by liver to urea and with enhanced tissue breakdown due to hemorrhage, trauma, or glucocorticoid therapy. • By comparison, a low protein diet or liver disease can lower the BUN without change in GFR. • Thus, liver disease may be associated with near normal values for both the BUN (due to decreased urea production) and the serum creatinine (due to muscle wasting) despite a relatively large reduction in GFR
in states of decreased effective intravascular volume, low urine tubular flow, and increased antidiuretic hormone, urea reabsorption can be substantial • less useful than the serum creatinine because the BUN can change independently of the GFR • Urea clearance underestimates GFR. • mean of creatinine and urea clearance would be a reasonable estimate of GFR
Serum cystatin C • low molecular weight protein that is a member of the cystatin superfamily of cysteine protease inhibitors. • Cystatin C is filtered at the glomerulus and not reabsorbed. • However, it is metabolized in the tubules, which prevents use of cystatin C to directly measure clearance. • Cystatin C is believed to be produced by all nucleated cells. Its rate of production has been thought to be relatively constant, and not affected by changes in diet, although this is not proven
cystatin C are affected by many factors other than GFR – inflammation, adiposity, thyroid, malignancy, steroids. • 2 studies - high levels in old age, male , fat , white, Dm, CRP , leukocytosis, low albumin • In multiple studies, serum cystatin C was more sensitive in identifying mild reductions in kidney function than serum creatinine alone
Nephron loss leads to compensatory hypertrophy and hyperfiltration in the normal or less affected nephrons. Because of this adaptive response, the GFR falls very little in mild kidney disease, and measurement of the creatinine clearance or use of an estimation equation will fail to detect the presence of disease. • Mild kidney disease may be detectable by abnormal findings in the urinalysis, such as hematuria and/or proteinuria.
protein • urine dipstick primarily detects albumin but not other proteins, such as immunoglobulin light chains. • This test is highly specific, but not very sensitive for the detection of proteinuria; it becomes positive only when protein excretion exceeds 300 to 500 mg/day. • insensitive method to detect microalbuminuria, which is the earliest clinical manifestation of diabetic nephropathy and is associated with increased cardiovascular risk in patients with and without diabetes • Dilute urine-underestmates and vise versa
Sulfosalicylic acid test — In contrast to the urine dipstick, SSA detects all proteins in the urine • A significantly positive SSA test in conjunction with a negative dipstick usually indicates the presence of nonalbumin proteins in the urine, most often immunoglobulin light chains. • Similar to the urine dipstick, radiocontrast agents can cause false positive SSA results • 24hr urine protein accurate • urine p/cr
Hematuria • High negative predictive value • Dipsticks for hemoglobin can detect 1 to 2 RBCs per high powered field • Positive- could be false as well
Urine sediments • In a normal patient, for example, one high power field may contain 0 to 4 white blood cells and 0 to 2 red blood cells, may be observed in 10 to 20 low powered fields • Abnormal--red and white blood cells and casts, and epithelial cells or casts
Thank You Sophia arunselvan MD