Making an Impact: Essential Steps for Effective Data Collection in Palliative Care
260 likes | 380 Vues
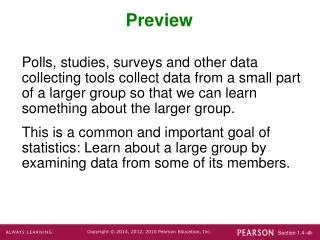
This comprehensive guide outlines crucial steps for collecting data in palliative care to enhance research, program development, and clinical assessment. Learn how to identify patient demographics, track outcomes, assess need for interventions, and evaluate financial metrics. Explore effective data collection sources and methodologies, including patient interviews, medical record reviews, and database management. Access insights to improve care quality, justify program expansions, and ensure effective communication with patients and families.

Making an Impact: Essential Steps for Effective Data Collection in Palliative Care
E N D
Presentation Transcript
Making an Impact: Simple Steps for Collecting Data R. Sean Morrison, MDDirector of Research, Hertzberg Palliative Care Institute, Mount Sinai School of Medicine Philip H. Santa-Emma, MD FAAHPM Chief Medical Director, Palliative Care Services Mount Carmel Health System
Why Collect Data? • Research • Programmatic development • Needs assessment • Making the case • Program maintenance • Continued justification • Expansion • Clinical assessment • Quality improvement
What Are The Variables? • Who are your patients? • What do they experience • What happens to them? • What do you do for them? • What do they cost? In other words…
Who are your patients? • Patient demographics and characteristics • Age • Sex • Diagnoses • Functional status • Next of kin (contact) • Referring physician • Advance directive status at time of consult • Presence and timing of DNR orders • Pain and other symptoms • Outcomes • In-hospital death rate, ICU death rate, length of stay • Discharge outcomes, ie hospice referrals
What happens to them? • Pain and other symptoms • Outcomes • In-hospital death rate • ICU death rate • Length of stay (hospital and ICU) • Discharges-continuum of care
What do you do for them? • Impact of palliative care • Hospital discharge • Transfer out of ICU • Advance care planning/DNR discussions • Palliative care interventions • Patient/Family/Physician satisfaction
What do they cost? • Financial Outcomes • Length of stay • ICU length of stay • Length of stay after palliative care consultation • Costs • Total costs, direct costs, pharmacy costs, ancillary charges
What Are The Data Sources? • Patients • Proxies • Family members, friends, health care professionals • Medical record review • Hospital databases
What Do You Need to Ask/Gather From Patients? • Demographic Information • Contact information, name/telephone number of proxy respondent • Demographics? • Age, sex, race, religion • Functional status • Karnofsky/PPS performance score, ADLs IADLs • Advance directive status • Health care proxy, living will, DNR, verbal directives • Pain and symptom assessment
What Do You Need to Ask/Gather From Proxies? • “Satisfaction” data • Identification of quality measures for your program • Processes of care • Outcomes
What Do You Need to Gather From The Medical Record? • Advance directive documentation • Living will, health care proxy, presence and timing of DNR orders • Site of hospital discharge, referral to hospice • Diagnoses and comorbid illnesses • Pharmacy data • Palliative care “interventions”
What Do You Need to Gather From Databases? • Patient characteristics and demographics • Age, sex, insurance status, DRG, diagnostic and procedure codes • Length of stay (ICU and hospital) • Costs (ancillary, pharmacy) • Pharmacy data (if available) • Analgesics, Antiemetics, Laxatives, Antidepressants, Anxielytics
Choosing Your Instruments: Measurement • Standardized progress notes • Patient interview form/Chart abstraction instrument • Team audit instrument • Post-discharge/death patient family satisfaction • Palliative Care Outcomes Scale • DART (Interviewer script, Interview) • Famcare
Setting Up Your Database • Necessary • “Database” options: • Spread sheets (Excel, Lotus, Quattro) • Patients are rows • Variables are columns • Statistical packages (SAS, Stata, SPSS) • Databases (MS Access/Filepro/SQL) • Simple forms that mimic your paper forms • Data stored in corresponding tables
How to setup a database • How to start • Simple spreadsheets can be setup with minimal computer knowledge • Simple databases can also be setup • Contact your computer department and use their expertise • Hire a private consultant
How to setup a database • How to enter information • Entered daily or after a patient’s discharge • Completion of missing or incomplete data • Storage of paper instruments
Data extraction • After data is entered, must be able to extract the information • Weekly or monthly ‘canned’ reports to look at basics, i.e. diagnosis, prior unit in the hospital, LOS, symptoms and outcomes • Specific queries run as needed, ‘how many patients with lung cancer from the ICU that were discharged home with hospice’
Most important • Backup data regularly! • Store paper records safely • Secure data to limit access
Palliative Care Program Patient Characteristics (1997-2000) • Median Age 71.4 (range 18 to 104) • 54% Women • 48% White, 23% African American, 23% Latino, 5% Other • 63% Medicare • 25% of all hospital deaths • Performance status at time of consult: • Moribund 17% • Very sick requiring active supportive treatment 32% • Severely disabled 26% • Disabled requiring assistance 14% • Normal activity but requiring frequent medical care 11% Source: palliative care database
Improvement in Symptoms for 2219 Patients Followed by the Palliative Care Service (6/97-12/02) Pain Nausea Severe Severe Mod. Mod. Mild Mild None None Shortness of Breath Anxiety Severe Severe Mod. Mod. Mild Mild None None
Percent of Palliative Care Families Satisfied or Very Satisfied Following Their Loved Ones Death With: • Control of pain - 95% • Control of non-pain symptoms - 92% • Support of patient’s quality of life - 89% • Support for family stress/anxiety - 84% • Manner in which you were told of patient’s terminal illness - 88% • Overall care provided by palliative care program- 95% Source: Post-Discharge/Death Family Satisfaction Interviews
Palliative Care Recommendations Forego Life Sustaining Treatment Source: Team Audit
Mount Sinai Hospital 2002: Savings for Medicare Beneficiaries Resulting From Palliative Care Consultation Day palliative care consultation obtained (median) Palliative Care Versus Non-palliative Care Patients Who Died Matched By Age/DRG For the 21 Days Prior to Death For 2002
Effect of a Palliative Care Inpatient Unit on Costs at Virginia Commonwealth University, Massey Cancer Center Approx. $700/day decrease in cost/day Source: T.J. Smith, MD, et al, VCU Massey Cancer Center, manuscript, “Palliative Care Unit Costs”, 2002, NOT FOR FURTHER DISTRIBUTION OR REPLICATION WITHOUT AUTHOR’S PERMISSION.
Summary and Discussion • Data are essential for programmatic justification, maintenance, clinical care, and quality • Target different sources for data collection • Patient, proxy, medical record, databases • Select sources based upon institutional resources • Use standardized instruments • Electronically store your data • Use data to support and convey your message