DEPRESSION
DEPRESSION. Alex Padikken 4 th Year Pharmacy Student Florida A&M University Disease State presentation. Objective. Define Depression Discuss the signs and symptoms Discuss risk factors, prevalence and pathophysiology Describe the components of diagnosis and treatment options. .


DEPRESSION
E N D
Presentation Transcript
DEPRESSION Alex Padikken 4th Year Pharmacy Student Florida A&M University Disease State presentation
Objective • Define Depression • Discuss the signs and symptoms • Discuss risk factors, prevalence and pathophysiology • Describe the components of diagnosis and treatment options.
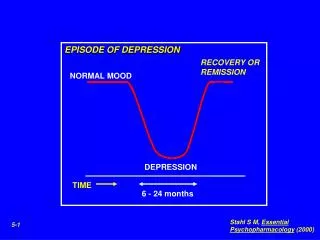
Definition • Depression is defined as intense feelings of sadness, mental slowing, hopelessness, despair, pessimistic worry, agitation, self-deprecation and inability to experience pleasure during usual activities.
Prevalence • 6.7% of US adults experience major Depressive disorder each year. • Women are 70% more likely than men to experience depression. • Average age of onset is 32 years old. • Non-Hispanic blacks are 40% less likely than Non-Hispanic whites to experience Depression.
Signs and Symptoms Decreased energy Difficulty concentrating Appetite loss Insomnia Thoughts of suicide • Fatigue • Feeling of Hopelessness • Feeling “empty” • Irritability • Restlessness
Risk Factors • Gender: Female • Having biological relatives with Depression • Abusing alcohol or any illicit drugs • Having traumatic experiences as a child • Depressed previously • Having serious medical conditions such as Parkinson's disease, dementia, stroke, HIV/Aids.
Etiology • The cause of depression are not well understood. • Combination of genetic, biologic and environmental factors.
Pathophysiology • Due to an alteration in neuronal and synaptic catecholamine concentration at adrenergic receptor sites in the brain, deficiency of catecholamine, especially NE and 5-HT
Depression Diagnosis • DSM IV • Diagnostic and statistical manual of mental disorder • At least five symptoms from the following list during the same two week period • Depressed mood • Marked diminished interest • Significant weight loss or weight gain • Insomnia or hypersomnia • Psychomotor agitation or retardation • Fatigue or loss of energy • Feelings of worthlessness • Diminished ability to concentrate • Recurrent suicidal ideation
Types of Depression • Major Depression • Dysthymic Disorder • Minor Depression • Postpartum Depression • Seasonal affective Depression
Major Depression • Combination of symptoms interfering a person’s ability to: • Work • Sleep • Study • Eat • Pleasurable activities
Dysthymic Disorder Minor Depression Characterized by having symptoms for 2 weeks or longer that do not meet full criteria for major depression. • Characterized by long term symptoms that prevents a person's normal functioning or well being.
Postpartum Depression Seasonal affective Depression (SAD) This type of depression is related to changes in seasons. • This is a common type of depression that occurs in new mothers. It often occurs between two weeks and six months after delivery.
Non-Pharmacological Treatment • St. John’s Wort • Not approved by FDA • Classified as a dietary supplement • Associated with many significant drug interactions • Omega 3 fatty acids • Supplement may ease depression • Used in addition to other standard depression treatment.
Non-Pharmacological Treatment • Psycotherapy • Cognitive-behavioral therapy (CBT) • Interpersonal therapy (IPT) • Electroconvulsive Therapy • Formerly known as “shock” therapy.
Treatment Options • SSRI • SSRIs block the reabsorption of the neurotransmitter serotonin in the brain • Most commonly prescribed antidepressants. • Ease symptoms of moderate to severe depression • Relatively safe and fewer side effects. • Citalopram (Celexa) • Escitalopram (Lexapro) • Fluoxetine (Prozac) • Paroxetine (Paxil) • Sertraline (Zoloft) • Fluoxamine (luvox) SIDE EFFECTS: reduced sexual desire, weight gain or weight loss, N/V, GI issues.
Treatment Options • SNRI • block the absorption of the neurotransmitters serotonin and norepinephrine in the brain. • Effective at easing depressive symptoms • Similar to SSRI • Duloxetine (Cymbalta) • Venlafaxine (Effexor XR) • Desvenlafaxine (Pristiq) SIDE EFFECTS: N/V, Sexual dysfunction, dry mouth, also increase BP.
Treatment Options • Tricyclics • Block the absorption of the neurotransmitters serotonin and norepinephrine • Block Ach and histamine receptors • Earliest antidepressants developed • Adjunctive analgesics for chronic pain conditions, such as trigeminal neuralgia • Childhood enuresis (imipramine) • Amitriptyline (elavil) • Desipramine(Norpramin) • Doxepin (sinequan) • Imipramine (Tofranil) • Nortriptyline (Pamelor) • Protriptyline (Vivactil) • Trimipramine (Surmontil) SIDE EFFECTS: Dry mouth, blurred vision, urinary retention, constiption, weight gain, vivid dreams
Treatment Options • MAO-Is • Inhibit MAO and cause accumulation of 5- HT, NE and DA in CNS and Periphery • Highly effective • Disadvantage: potential to cause hypertensive crisis when taken with tyramine • Use is limited due to dietary restrictions • Isocarboxazid(Marplan) • Phenelzine (Nardil) • Selegiline (Emsam) • Tranylcypromine (Parnate) SIDE EFFECTS: Dry mouth, headache, dizziness, drowsiness, insomnia
Additional Agents • Bupropion (Wellbutrin) • Mirtazapine (Remeron) • Trazodone (Oleptro) • Nefazodone • DA and NE reuptake inhibitors • NE and 5HT reuptake inhibitors • Inhibits 5HT reuptake and alpha 1-adrenergic and histamine blocker • Similar to Trazadone but less sedating and increased risk of hepatotoxicity
Special Population • Pediatric Patients • Childhood depression is very common • Only FDA approved medication is Fluoxetine • Elderly patiets • SSRIs are the first line therapy • Age 65 and older have the highest suicide rate
Clinical pearls • All antidepressant comes with a black box warning • Benefit of the medication start within 1-2 weeks • It takes 6-8 weeks to see the full drug effect • SSRIs and SNRIs are considered first line treatment options
Pharmacist Role • Dispense Medication Guide and instruct patients to read it • Counsel on lag time and the need to take it daily as with other agents • Counsel the patients on side effects • Counsel the patient to avoid abruptly discontinuing the antidepressants without consulting the physician.
References • Mann JJ. The Medical Management of Depression. N Engl J Med 2005;353:1819–1834. • O'Connor EA, Whitlock EP, Beil TL, Gaynes BN. Screening for depression in adult patients in primary care settings: a systematic evidence review.Ann Intern Med . 2009 Dec 1;151(11):793-803. • Association AP. Practice guideline for the treatment of patients with major depressive disorder (revision). American Psychiatric Association. Am J Psychiatry 2000; 157: 1-45. • U.S. Preventive Services Task Force. Screening for depression in adults: U.S. preventive services task force recommendation statement. Ann Intern Med . 2009 Dec 1;151(11):784-92. • Staff, Mayo Clinic. "Definition." Mayo Clinic. Mayo Foundation for Medical Education and Research, 10 Feb. 2012. Web. 02 Oct. 2013. • Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials.JAMA . 2007 Apr 18;297(15):1683-96.