Download
1 / 43
440 likes | 681 Vues
Diagnosis of Cushing’s Syndrome. David W Ray FRCP PhD , University of Manchester Professor of Medicine and Endocrinology. Cushings syndrome. Harvey Cushing 1912 50% 5 year survival Glucocorticoid excess Iatrogenic Pituitary ACTH Ectopic ACTH Primary adrenal (ACTH independent).

E N D
Diagnosis of Cushing’s Syndrome David W Ray FRCP PhD, University of Manchester Professor of Medicine and Endocrinology
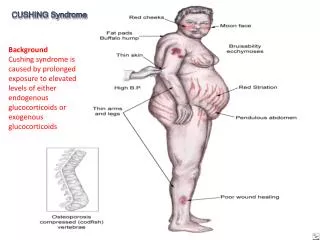
Cushings syndrome • Harvey Cushing 1912 • 50% 5 year survival • Glucocorticoid excess • Iatrogenic • Pituitary ACTH • Ectopic ACTH • Primary adrenal (ACTH independent)
Cushings disease • Pituitary ACTH producing adenoma • 70% of adult Cushings • Female:male 3:1 up to 10:1 • Age 25-45 • Incidence ? 1 per 100,000 per year (RARE)
Clinical features • Central obesity (fat re-distribution) • Protein wasting (osteoporosis, myopathy) • Plethora • Acne • Striae (red, purple) • Hypertension (diastolic >105) • Oedema • Hirsutism • Bruising • Hypokalaemia
Clinical features NOT discriminating • Generalised obesity • Oligomenorrhoea • Headaches • Abnormal GTT
Difficult diagnoses • One symptom may predominate • Severity of disease (mild disease-less florid clinical features) • Fluctuating cortisol secretion, cyclical Cushings • Male gender (? Confounding effects of testicular androgens)
Diagnosis • Suspect it! • Confirm hypercortisolaemia • Identify the source • Planned, coordinated investigation essential • Access to dedicated in-patients beds, trained nurses, lab support, modern imaging • May take time!!
Hypercortisolaemia • Plasma cortisol (am vs pm vs midnight sleeping) • Salivary cortisol • Urine collection (urinary free cortisol) • Dynamic tests • O/N Dex suppression test • Low dose,2 day Dex suppression test
Urinary cortisol • 24 hour collection: complete collection-loss of collection depends on timing • Overnight collection • Good distinction between normals and Cushings • Sensitive • Need repetition • Repeated normal tests unlikely in Cushings • “Raised” UFC obesity, PCOS, depression
Plasma cortisol • 9am cortisol, significant overlap with normals • 8-9pm cortisol 10-15% overlap • Midnight sleeping cortisol 50nM/l separates normals from Cushings • Acclimatise patients to inpatient stay, in patient costs, timing of sample, stress free sample
Salivary cortisol • Sample collection • RIA, ELISA, Platform, LC/MS • Late night salivary cortisol highest sensitivity for diagnosis of Cushings • Raff JCEM 2009: 94;3647-3655 Two late night salivary cortisol measurements sensitivity 92%, specificity 96%
Salivary cortisol • Correlates with free serum cortisol • CBG raised with oestrogens (eg OCP) • CBG suppressed in illness (eg medical inpatients) • ELISA cross-reacts with cortisone, and prednisolone • ? Advantages in measuring salivary cortisone??
IV physio: correlations in all groups SerF-SalF ALL FreeF-SalF ALL SerF-FreeF ALL r=0.64 400 r=0.8 300 400 300 300 200 200 200 FreeF (nmol/L) SalF (nmol/L) 100 100 100 0 0 500 1000 1500 2000 2500 0 100 200 300 SerF (nmol/L) 0 500 1000 1500 2000 2500 -100 SerF (nmol/L) -100
Suppression tests • Overnight 1mg Dex supp test: • 1mg Dex at 11pm, serum cort at 8am • Timing, compliance, metabolism (drugs) • Threshold (<50 nM/l) • 13% obese, 23% hospitalised false positive • Low dose, 2 day test • 0.5mg Dex every 6 hours for 2 days • Serum cort at 9am day 0 and 9 am day 2 • Cort <50nM/l • >95% sensitivity and specificity • Useful as a confirmatory test
Screening tests • x2 salivary cortisol • Confirmatory 48 hour LD dex suppression test (?as OP)
Cushings • ACTH dependent or not • Measure ACTH when confirmed hypercortisolaemia • If ACTH is easily detectable (ie normal range or raised) ACTH dependent • Low ACTH compatible with primary adrenal causes (nodular adrenocortical hyperplasia); • NB ACTH vs other peptides, assay performance, low ref ranges
ACTH dependent • Pit vs ectopic • Aggressive ectopics usually obvious (CXR, systemic features) • Small ectopics can mimic pit adenoma • Pit can have adenomata incidentally • Use dynamic tests, imaging, and venous sampling • Time and patience required!!
High Dose Dex suppression • Pre ACTH assay means to differentiate adrenal from pituitary ACTH dependent • 2mg Dex exactly every 6 hours • Measure cortisol at 9am days 0,1 and 2 • 10% false +ve • 10% false –ve • [circa 70+ % pituitary anyway]
CRH test • Overnight admission • At 9am, insert cannula • Obtain 3-4 basal samples • IV CRH (human) 100ug • Serial samples after • Measure ACTH and cortisol • Define increment (>25% increase) • 10% false negative • 10% false positive
Combined Tests • High dose Dex and CRH • If either is positive, suggests pituitary • If both are negative, suggests ectopic • Grossman et al 1988; Clin Endocrinol 29:167-178
Venous sampling • Bilateral IPSS • Most useful test • Dependent on expertise • Labour intensive • Potentially dangerous • NOT a test for Cushings! • Only of use if patient is hypercortisolaemic at time of test
IPSS • All or selective? • Cannulate the inferior petrosal sinuses, and peripheral vein • Simultaneous sampling basally (repeated) • Inject 100ug CRH • Simultaneous sampling post injection • Concurrent cortisol measurements (UFC, midnight serum) to ensure disease activity
IPSS Peak post CRH Basal
Ectopic • Failed dynamic tests • Failed IPSS • Pit imaging pitfalls!! • Chest, pancreas, duodenum, adrenals, sympathetic chain • CT with contrast
Adrenal • ACTH independent • CT imaging • Unilateral vs bilateral
Treatment • Medical • Surgical • Radiotherapy
44 year old man • Orbital radiotherapy as a child for rhabdomyosarcoma • Opthalmic Graves • TSH 0.05, T4 48 (50-150) • Given T4 by GP • Now, BP90/?20, nausea, vomiting, weight loss, [Na] 120mmol/l • Diagnosis?
Adrenal Crisis • Sick patient, hypotension, hyponatraemia • Random serum cortisol and plasma ACTH • TREAT, high dose, replacement hydrocortisone • 100mg IV every 6 hours • Intravenous saline • 2-3 l first hour, then 3-4 l per day
Screening Tests; Not Acutely Sick • Morning plasma cortisol. • <140nM/l highly suggestive. • >415nM/l diagnosis unlikely. • Random levels >500nM/l make diagnosis unlikely.
Chronic Deficiency • High dose short Synacthen test • Convenient, catches are pituitary disease of recent onset. • Peak cortisol >550 nM/l (NB variation amongst cortisol assays). • Metyrapone test • In-patient test. Patients may become acutely hypoadrenal.
Chronic Deficiency • CRH test • Expensive, variable responses, rarely used. • ITT • Significant risk (CV disease, epilepsy), not for use in patients with high probability of adrenal insufficiency.
Treatment • Replacement of the missing steroid(s). • Primary adrenal disease: cortisol and aldosterone. • Pituitary disease: cortisol. • Hydrocortisone=cortisol. • Once a day, twice a day, three times a day. • Synthetic vs natural.
Treatment • Hydrocortisone 10, 5, 5mg • Waking, lunch, late pm • Longer acting steroids x1/day • Prednisolone 2.5-7.5mg • Dexamethasone 0.25-0.75mg • Single dose at night, or on waking • No evidence comparing these approaches
Monitoring • Clinical indices • Under replacement: • Weight loss, hyponatraemia, pigmentation • Over replacement: • Cushing’s syndrome (obesity/fat distribution, striae, hypertension, hyperglycaemia) • ? Changes in bone turnover/osteoporosis • Biochemical tests • Measure cortisol after Hc dosing
Hc Day Curves • Hc on rising (approx 7am) • Cortisol 9am, 12-30pm and 5-30pm; with 24hour UFC • UFC (<300nmol/24hour) ie normal range • 9am cortisol 100-700nM/l • 12-30pm, and 5pm >50nM/l; ideally >100nM/l • After Howlett
Adequacy of glucocorticoid cover • NB hepatic enzyme inducers: phenytoin, rifampicin, barbiturates require increased doses. • Intercurrent illness, patient education • Steroid card and medic alert bracelet • Injection kit of hydrocortisone or dexamethasone
Surgery, major stress • Estimated cortisol production increases to 200ug/day • Therefore hydrocortisone 100mg iv/im every 6 hours. • Half daily dosage each day post op • Back to routine replacement by day 5-6 • There is evidence that this approach is unnecessary, but it remains standard practice!