Download
1 / 26
260 likes | 549 Vues
Weight loss Surgery. Kuldeep Singh, M.D., F.A.C.S., M.B.A. Spectrum of the obesity. Terms Used to Describe Various Levels of Body Fat. Normal Weight (BMI 18.5 to 24.9). Overweight (BMI 25 to 29.9). Obese (BMI 30 to 34.9). Severely Obese (BMI 35 to 39.9 ). Morbidly Obese (BMI 40 or more).

E N D
Weight loss Surgery Kuldeep Singh, M.D., F.A.C.S., M.B.A.
Spectrum of the obesity Terms Used to Describe Various Levels of Body Fat Normal Weight (BMI 18.5 to 24.9) Overweight(BMI 25 to 29.9) Obese(BMI 30 to 34.9) Severely Obese(BMI 35 to 39.9 ) Morbidly Obese(BMI 40 or more) This is where Surgical treatment is recommended
Health Risks Related Diseases and Health Problems • Obese people have more risk for: • Diabetes (type 2) • Joint problems, backaches, disc Prolapse (e.g., arthritis) • High blood pressure • Heart disease: coronary artery disease • Gallbladder problems, gallstones Source: The Surgeon General’s Call to Action to Prevent Overweight and Obesity.
Health Risks (cont.) Related Diseases and Health Problems • In addition, obese people have more risk for: • Certain types of cancer (breast, uterine, colon) • Digestive disorders (e.g. gastro-esophageal reflux disease, or GERD) • Breathing difficulties (e.g. sleep apnea, asthma). • Psychological problems such as depression. • Problems with fertility and pregnancy. • Stress Incontinence. Source: The Surgeon General’s Call to Action to Prevent Overweight and Obesity.
Using Surgery to Treat Obesity • Types of weight-loss surgeries • Malabsorptive procedures shorten the digestive tract: BPD & BPD-DS • Restrictive procedures reduce how much the stomach can hold: Lap Band & Sleeve Gastrectomy • Combined procedures shorten the digestive tract and reduce how much the stomach can hold: Gastric Bypass
Using Surgery to Treat Obesity- Restrictive Techniques Sleeve Gastrectomy LAP-BAND System wo-pub2.med.cornell.edu/.../PublicA.woa/4/wa
Using Surgery to Treat Obesity- Malabsorptive Techniques We do not perform BPD, however we can refer you to surgeons in the area who perform this surgery Bilio-Pancreatic Diversion (BPD)
Risk Benefit Ratio LOW LOW Riskier the operation, the more effective it is Lap Band Lap Band Sleeve Gastrectomy Sleeve Gastrectomy Roux –en-Y Gastric Bypass Roux –en-Y Gastric Bypass Bilio-Pancreatic Diversion Bilio-Pancreatic Diversion HIGH HIGH RISK BENEFIT
Expected Outcomes from the Surgery • Improvement in health problems, including: • Diabetes (type 2): 80% cure possible. • High blood pressure: 40% cure • Asthma: marked improvement • GERD (gastro-esophageal reflux disease): • Sleep apnea: close to 100% cure • Problems with fertility and pregnancy • Depression.
Advantages Rapid initial weight loss Higher total average weight loss . Over 40 years of surgical experience in USA Disadvantages Bigger operation and slower recovery. Practically irreversible Higher chances of nutritional problems such as Iron deficiency anemia and vitamin B 12 deficiency. Higher chances of ulcers at the junction of the stomach and the jejunum. Laparoscopic Gastric Bypass
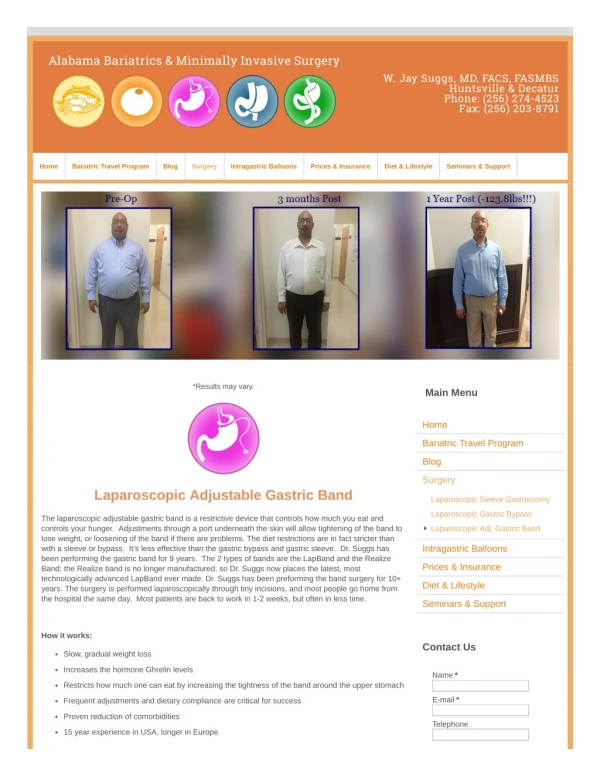
How the LAP-BAND System Works • A siliconeband is placed around the upper part of the stomach • A small pouch is created • Your stomach holds less food • You feel full faster and longer
The LAP-BAND System Procedure • Adjustable Band • Can be adjusted in office or operating room • No anesthesia needed. • On average 4-5 fills in first year • 1 or 2 fills second year if needed.
Advantages Lowest mortality rate No stomach stapling or cutting, or intestinal re-routing Adjustable Smaller operation , Reversible Lowest operative complication rate Low malnutrition risk Disadvantages Slower weight loss. Regular follow-up critical for optimal results Requires more commitment from the patient. Slippage or erosion and injury to the esophagus or stomach as possible complications. The LAP-BAND System
Sleeve Gastrectomy (SG) • Arose from need to perform a safer yet effective operation in patients with high BMI (>50) and multiple co-morbidities. • It is first stage of BPD-DS (Bilio-pancreatic diversion with Duodenal switch). • Designed as an separate staged procedure by Johnson in 1993.
Sleeve Gastrectomy • Complications and outcomes are somewhere between Adjustable Laparoscopic gastric Banding and Gastric Bypass. • Advantage of absence of Iron deficiency anemia, Marginal Ulcers, ability to perform upper endoscopic procedures and decrease the weight and co-morbidities to lead to any second staged procedure such as band, bypass or BPD.
Who qualifies for the Bariatric Surgery? • NIH criteria • Weight: BMI more than 40 or 35 with two serious illnesses. • Free from untreated mental illnesses such as Bulimia and schizophrenia. • Documented evidence of weight loss attempts. In Maryland 6 months over the past two years. • Understanding by the patient that the surgery is only a tool to lose weight and need to have life style changes and exercise/ eating habits. • Age: 18-60 years of age
Who does not qualifies for the Bariatric Surgery? These are our contraindications • Those who cannot walk. • Those who have severe heart disease. • Heart failure. • Angina and coronary artery disease. • With severe lung disease. • In whom surgery is not possible • Extreme obesity. Absolute weight matters to an extent. I will not operate patients over 500 lbs. • Limited exercise tolerance. You should be able to walk with me to the parking lot (2 blocks) and back without severe shortness of breath. • Schizophrenia and Bulimia.
Bypass or Band?? How to choose?some guidelines • Bypass • Bigger operation, higher risk, more weight loss and rapid weight loss. • More nutritional problems: anemia and ulcers. • My preference: severe obesity with lot of illnesses. • Lap Band • Smaller and safer surgery, quick recovery. • Less nutritional problems, less anemia or ulcers. • Unique problems such as Slippage and Erosions. • Reversible. • My preference: BMI small with not so many diseases, women. • Sleeve Gastrectomy • BMI>60. • Android Obesity
The process for the surgery • Make sure you meet the criteria for the surgery. • Call your insurance company to check coverage. • Make sure that we participate with your insurance or be willing to pay more out of Pocket expense. • See the dietician and the psychologist. • Fill all the forms and organize your folder into weight loss attempts, cardiac consult , Sleep Study and History and physical note form your doctor (whatever applies). • Call the office and make appointment to see the Doctor. • If you have questions whether you will qualify- Call the office to clarify.
Centers of Excellence • Awarded COE by most of the Insurers in Maryland (Blue cross, Atena, United Healthcare and Cigna). • Awarded COE by SRC (Surgical review Committee in June 2006 for full three years.
Morbidity and Mortality of Gastric Bypass surgery at St. Agnes Hospital 2001-2007
Comparison of % EBWL of Gastric bypass and Lap. Band patients Chapman et al.; Surgery 135:326-351: 2004
Resolution of co-morbidities after 1 year in Gastric bypass patients with Insurance mandated diet Jamal et al., SOARD 2:122-127; 2006