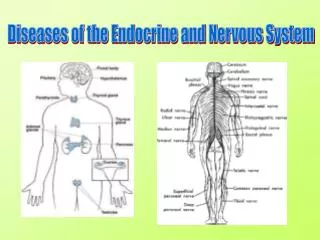
Behavioural changes in endocrine diseases
290 likes | 462 Vues
Behavioural changes in endocrine diseases. DIABET ES INSIPID US. DIABET ES INSIPID US. Diabetes insipidus is a disorder of a large volume of urine (diabetes) that is hypotonic, dilute, and tasteless (insipid). This is opposed to the hypertonic and sweet urine of

Behavioural changes in endocrine diseases
E N D
Presentation Transcript
DIABETES INSIPIDUS Diabetes insipidus is a disorder of a large volume of urine (diabetes) that is hypotonic, dilute, and tasteless (insipid). This is opposed to the hypertonic and sweet urine of diabetes mellitus (honey). Definition: polyuria-thirst- polydipsia(>3l/24h) associated with urine hypoosmolality (<300mOsm/l)
Clinical characteristics • sudden onset of symptoms • persistent thirst throughout the day and night • associated with a desire for cold liquids
Classification of diabetes insipidus • Vasopressin (AVP) and oxytocin are synthesized in the magnocellular neurons of the supraoptic and paraventricular nuclei. • They migrate along the axons of the magnocellular neurons, to be stored and released at the ends of the neuronal tracts. • Renal action
The physiologic regulation of vasopressin synthesis and secretion involves two systems: Osmotic and Pressure/volume • Pressure/volume • High pressure arterial baroreceptors are located in the carotid sinus and aortic arch and • Low pressure volume receptors are located in the atria and pulmonary venous system. • The afferent signals are carried through cranial nerves IX and X. • When the hypovolemia is sufficient to cause a decrease in blood pressure (5-10%), there is a sudden and exponential increase in the level of vasopressin in plasma
Osmotic system • The primary receptors for sensing changes in osmolality are located in the brain. • !Osmoreceptors must be outside the blood-brain barrier. • Primary osmoreceptors: organum vasculosum of the lamina terminalis (OVLT) and areas of the anterior hypothalamus
Extracellular fluid osmolality (predominantly determined by sodium concentration) varies from 280 to 295 mOsm/kg H2O in normal subjects but in any individual is maintained within a narrow range. • As little as a 1% increase or decrease in plasma osmolality will cause a rapid increase/decrease in plasma vasopressin by release of vasopressin from the store of hormone in the posterior pituitary. • When vasopressin is absent, 18 to 20 L/day are excreted, but with an increase to as little as 0.5 to 1 pg/mL, urine volume is reduced to less than 4 L/day.
Thirst • Represents the body's defense mechanism and water consumption is increased in response to perceived deficits of body fluids. • As with to vasopressin, increases in osmolality of the extracellular fluid (ECF) or decreases in intravascular volume can stimulate thirst. • ! Most humans consume the bulk of their ingested water as a result of the relatively unregulated components of fluid intake, such as • the consumption of beverages in association with food intake, • for reasons of palatability or • for desired secondary effects (e.g., caffeine), or • for social or habitual reasons (e.g., sodas or alcoholic beverages);
Sexual hormones Hypogonadism=sexual hormones deficiency • In children : delayed puberty • In women: chronic anovulation, amenorhoeae, infertility, reduced libido, genitourinary atrophy, osteoporosis • In men: reduced libido, impotence, reduced muscle mass, increased fat, osteoporosis, lethargy, reduced testicular volume, hypospermia, hair loss, fine wrinkling
Androgen excess • Such cases may present in early childhood with signs of precocious pseudopuberty such as sexual precocity, pubic hair development, and/or growth acceleration due to premature androgen excess.
GLUCOCORTICOIDS • Clinical observations on patients with glucocorticoid excess and deficiency reveal that the brain is an important target tissue for glucocorticoids, with depression, euphoria, psychosis, apathy, and lethargy being important manifestations. • Both glucocorticoid and mineralocorticoid receptors are expressed in discrete regions of the rodent brain, including hippocampus, hypothalamus, cerebellum, and cortex. • Glucocorticoids cause neuronal death, notably in the hippocampus,which may underlie the recent interest in glucocorticoids and cognitive function, memory, and neurodegenerative diseases such as Alzheimer's.
GLUCOCORTICOIDS • Central action on circuits involved in energy homeostasis • GC simulate hunger and weight gain • Hypercortisolism => central fat distribution
Features of chronic adrenal insufficiency • Weakness, tiredness, weight loss, nausea, intermittent vomiting, abdominal pain, general malaise, muscle cramps, and symptoms suggestive of postural hypotension • Psychiatric symptoms may occur in longstanding cases and include memory impairment, depression, and psychosis. • Patients may be inappropriately diagnosed as suffering from chronic fatigue syndrome or anorexia nervosa.
Deficiency of thyroid hormone in adult life • Causes less severe manifestations that usually respond to treatment with the hormone. • All intellectual functions, including speech, are slowed in thyroid hormone deficiency. • Loss of initiative is present, memory defects are common, lethargy and somnolence are prominent, and dementia in elderly patients may be mistaken for senile dementia. • Psychiatric disorders are common and are usually of the paranoid or depressive type and may induce agitation (myxedema madness). • Cerebral hypoxia due to circulatory alterations may predispose to confusional attacks and syncope, which may be prolonged and lead to stupor or coma.
Hormonii necesită concentraţii optime pentru determinismulcomportamental • Modificările SN şi comportamentale: • letargie, astenie fizică, scăderea atenţiei şi gândirii, tulburări de memorie, încetinire mentală, bradilalie şi ezitări în vorbire, depresie, diminuarea auzului, somnolenţă • rar: sindroame neurologice, reversibile la tratamentul de substituţie tiroidiană, disfuncţie cerebelară cu ataxie, tremor de intenţie şi nistagmus ♀, 65 ani, mixedem La vârstnici: alterarea funcţiei cognitive şi simptome depresive
Congenital myxedema • Thyroid hormone is essential for the development of the central nervous system. Deficiency in fetal life or at birth impairs neurologic development, including hypoplasia of cortical neurons with poor development of cellular processes, retarded myelination, and reduced vascularity. • ! If the deficiency is not corrected in early postnatal life, the damage is irreversible.
Alterations in the function of the nervous system in thyrotoxicosis • Are manifested by nervousness, emotional lability, and hyperkinesia. • Fatigue may be due to both the muscle weakness and the insomnia that are commonly present. • Emotional lability is common and in rare cases mental disturbance may be severe; manic depressive, schizoid, or paranoid reactions may emerge. • The hyperkinesia During the interview, the patient shifts positions frequently, and movements are quick, jerky, exaggerated, and often purposeless.
Hormonii necesită concentraţii optime pentru determinismulcomportamental • Manifestări SN şi comportamentale: • nervozitate, iritabilitate, labilitate emoţională, anxietate persistentă, nelinişte, senzaţie de tensiune interioară, instabilitate în modul de a fi, somn neodihnitor, insomnii, scăderea puterii de concentrare, tulburări de memorie, fugă de idei, delir • reacţie exacerbată în situaţii stresante ♀, 22 ani, boală Graves Basedow
Thyrotoxicosis in children • In children, in whom such manifestations tend to be more severe, inability to focus may lead to deterioration of school performance, suggesting attention deficit hyperactivity disorder.
SIGNS AND SYMPTOMS ASSOCIATED WITH CATECHOLAMINE-SECRETING TUMORS • SPELL RELATED Anxiety and fear of impending death Diaphoresis Dyspnea Epigastric and chest pain Headache Hypertension Nausea and vomiting Pallor Palpitation (forceful heartbeat) Tremor