The Anus and Rectum
One of the truly incredible properties of the anal canal is its resistance to infection, as well as the ability of its mucosa to heal after surgical intervention despite the torrent of micro-organisms passing over it. The Anus and Rectum. Anatomy of anal canal .

The Anus and Rectum
E N D
Presentation Transcript
One of the truly incredible properties of the anal canal is its resistance to infection, as well as the ability of its mucosa to heal after surgical intervention despite the torrent of micro-organisms passing over it. The Anus and Rectum
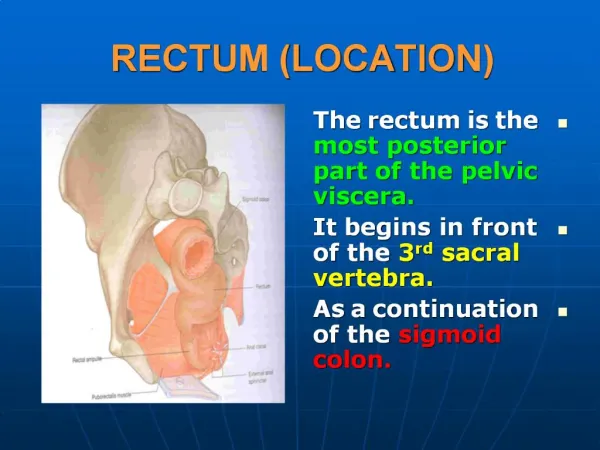
Anatomy of anal canal • The anal canal 4 cm from the anorectal ring to the hairy skin of the anal verge • Its lining, as well as its musculature, has important features that, together with the pelvic floor structures, contribute significantly to the regulation of defecation and continence. • Its borders include the coccyx posteriorly, the ischiorectalfossa and its contents bilaterally, and the perineal body and vagina in women and the urethra in men anteriorly.
Anal Canal Lining • The characteristically serrated dentate (or pectinate) line ismade up of anal valves. The proximal mucosa is corrugated into a series of 12 to 14 columns of Morgagniwith corresponding crypts between each fold. Opening into these crypts are a variable number of anal glands, which traverse the submucosa to enter the internal sphincter to terminate in the intersphincteric plane • The mucosa of the upper anal canal, like that of the rectum, is pinkish and is lined by columnar epithelium, whereas the mucosa distal to the dentate line is paler and lined by squamous epithelium devoid of hair and • Transitional zone, which lies immediately proximal to the dentate line, which is purplish in color. • At the anal verge, the lining acquires the characteristics of normal skin with its apocrine glands, and this is where infectious complications of the apocrine glands, hidradenitissuppurativa, present.
Anal Canal Musculature • The inner component is the continuation of the smooth circular layer of the rectum forming the thickened and rounded internal sphincter that ends 1.5 cm below the dentate line. • The outer component is a continuous sheet of striated muscle constituting the pelvic floor, which comprises the levatorani muscle, the puborectalis muscle, and the external sphincter .The latter is elliptical and engulfs the anal canal and the internal sphincter, beyond which it terminates in a subcutaneous portion.
The anorectal ring • The anorectal ring marks the junction between the rectum and the anal canal. It is formed by the joining of the puborectalis muscle the deep external sphincter, conjoined longitudinal muscle and the highest part of the internal sphincter. • The anorectal ring can be clearly felt digitally, especially on its posterior and lateral aspects.
Blood supply to the anal canal is via superior, middle and inferior rectal vessels • Lymphatic drainage of the lower half of the anal canal goes to inguinal lymph nodes
Pathogenesis • Within the normal anal canal exist specialized, highly vascularized “cushions” forming discrete masses of thick submucosa containing blood vessels, smooth muscle, and elastic and connective tissue. They are located in the left lateral, right anterior, and right posterior quadrants of the canal to aid in anal continence. • The term hemorrhoids should be restricted to clinical situations in which these “cushions” are abnormal and cause symptoms. • The cause of hemorrhoids remains unknown. They may be no more than the downward sliding of anal cushions associated with gravity, straining, and irregular bowel habits (1ry) . • Malignancy ,pregnancy and portal hypertension (2ry)
Classification • Hemorrhoids can be considered external or internal • External hemorrhoids are covered with anoderm and are distal to the dentate line; they may swell, causing discomfort and difficult hygiene, but cause severe pain only if actually thrombosed. External haemorrhoids relate to venous channels of the inferior haemorrhoidal plexus deep in the skin surrounding the anal verge and are not true haemorrhoids; they are usually only recognised as a result of a complication, which is most typically a painful solitary acute thrombosis. • External haemorrhoids associated with internal haemorrhoids (‘interoexternal piles’) result from progression of the latter to involve both haemorrhoidal plexuses and are best thought of as being external extensions of internal haemorrhoids. • Internal hemorrhoids cause painless, bright red bleeding or prolapseassociated with defecation. • Internal hemorrhoids are classified according to the extent of prolapse, which influences treatment options
Internal Hemorrhoids: Grading • First degree : Bleeding; no prolapse • Second degree: Prolapse with spontaneous reduction • Third degree :Prolapse requiring digital reduction • Fourth degree :Prolapsed, cannot be reduced or Strangulated
Clinical picture • The patient may report dripping or even squirting of blood in the toilet bowl. • Chronic occult bleeding leading to anemia is rare, and other causes of anemia must be excluded. • Prolapse below the dentate line area can occur, especially with straining, and may lead to mucus and fecal leakage and pruritus. • Pain is not usually associated with uncomplicated hemorrhoids . • The physical examination should include inspection during straining, digital rectal examination; and anoscopy . • Digital examination enables exclusion of low rectal or anal canal neoplasms. • Anoscopy is the definitive examination, but a flexible proctosigmoidoscopy should always be added to exclude proximal inflammation or neoplasia.
Treatment • Depending on degree of disease, treatment falls into two main categories: nonsurgical and hemorrhoidectomy. • Nonoperative In many patients, hemorrhoidal symptoms can be relieved by simple measures, such as Better local hygiene. Avoidance of excessivestraining. And better dietary habits. Supplemented by medication to keep stools soft.
Procedure • In the absence of symptomatic external hemorrhoids, second- and some third-degree internal hemorrhoids can be treated with office procedures. Although sclerotherapy, infrared coagulation, heater probe, and bipolar electrocoagulationall have been described, the simplest, most effective,and most widely applied office procedure is rubber band ligation. • Because severe perineal sepsis and even deaths have been reported after rubber band ligation, patients should be instructed to return to the emergency department if delayed or undue pain, inability to void, or a fever develops.
Surgical Treatment • Hemorrhoidectomy should be considered whenever patients fail to respond satisfactorily to repeated attempts at conservative measures; hemorrhoids are severely prolapsed and require manual reduction; hemorrhoids are complicated by strangulation or associated pathology, such as ulceration, fissure, fistula. • For simple thrombosed external hemorrhoids, excision is best performed early in the course of the disease, during the period of maximum pain. • Postoperative complications include fecal impaction, infection, urinary retention, and rarely arterial bleeding.
Complication of hemorrhoid • Bleeding • Strangulation • Gangrene • Infection • Portal pyeamia • Thrombosis
Treatment of complications • Strangulation, thrombosis and gangrene In these cases it was formerly believed that surgery would promoteportal pyaemia. However, if adequate antibiotic cover is given from the start, this is not found to be so. The other risk if surgery is performed at this stage, that of postoperative stenosis, results in some surgeons reviewing the situation much later and carrying out haemorrhoidectomy only if necessary. Besides adequate pain relief, bed rest with frequent hot baths and warm or cold saline compresses with firm pressure usually cause the pile mass to shrink considerably in 3–4 days. • Severe haemorrhage The cause usually lies in a bleeding diathesis or the use of anticoagulants. If such causes are excluded, a local compress containing adrenaline solution, with an injection of morphineand blood transfusion if necessary, will usually suffice. However, after adequate blood replacement, ligation and excision of the piles may be required.
Anal Fissure • An anal fissure is a linear ulcer of the lower half of the anal canal, usually located in the posterior commissure in the midline . • Location may vary, and an anterior midline fissure is seen more often in women. • Characteristic associated findings include a sentinel pile or tag externally and an enlarged anal papilla internally. • Fissures away from these two locations should raise the possibility of associated diseases, especially Crohn’s disease. • Because it involves the highly sensitive squamous epithelium, fissure in ano is often a painful condition. With defecation, the ulcer is stretched, causing pain and mild bleeding.
Pathogenesis • Many factors appear likely, such as the passage of large, hard stools, which may be the initiating factor; inappropriate diet; previous anal surgery; childbirth; and laxative abuse. • Higher than normal resting anal canal pressures and reduced anal blood flow in the posterior midline. It is therefore believed that anal fissures are the result of anal sphincter hypertoniaand subsequent mucosal ischemia.
Clinical picture • The diagnosis is secured by the typical history of pain and bleeding with defecation, especially if associated with prior constipation and confirmed by inspection after gently parting the posterior anus. • Digital as well as proctoscopic examination may trigger severe pain, interfering with the ability to visualize the ulcer. An endoscopic examination should be performed, but it can be delayed 4 to 6 weeks, until the pain is resolved with medical management or until surgery is performed for those cases refractory to medical therapy
Differential Diagnosis • Crohn disease • Anal tuberculosis • Anal malignancy • Abscess • Fistula • Cytomegalovirus
Medical Management • Gaining in popularity, particularly for acute fissures, that is, those presenting within 3 to 6 weeks of symptom onset. • The traditional first-line therapy for acute fissures is treatment with warm Sitz baths and bran or bulking agents, with rates of fissure healing reported as 87%. • Hydrocortisone and lidocainehave been advocated as local topical therapies for acute fissures. • Patients with chronic fissures should be started on the acute fissure regimen but are typically also started on other therapies simultaneously, including nitroglycerinor isosorbidedinitrateproducing“reversible chemical sphincterotomy.” by reducing spasm, pain is relieved, and increased vascular perfusion promotes healing. Such agents include glyceryltrinitrate (GTN) 0.2% applied four times per day to the anal margin (although this may cause headaches) and diltiazem 2% applied twice daily. • Internal sphincter injection of botulinum toxin
Surgical Treatment • Patients with chronic fissures who fail medical therapy either for persistent or recurrent. • Partiallateral internal sphincterotomy. • An alternate surgical approach is the anorectal advancement flap. • The flap procedure is particularly attractive for patients with low anal pressures, that is, those who have failed previous sphincterotomy despite a postoperative lowering of anal pressure, and for those with severe anal stenosis.
Anorectal Abscess • Infection originates in the intersphincteric plane, most likely in one of the anal glands. This may result in a simple intersphincteric abscess, or it may extend vertically either upward ,downward, or circumferentially resulting in a number of clinical presentations. • Severe anal or perianal pain, usually continuous and throbbing
Clinical Presentation: • Types of Abscesses • An intersphincteric abscess is limited to the primary site of origin and may be asymptomatic or result in severe, throbbing pain that resembles the pain of a fissure but it is persistent even without dification . Presents as a tender swelling, which can be misinterpreted as a thrombosed external hemorrhoid. • If the infection spreads vertically upward, an intermuscular abscess within the rectal wall or a supralevator abscess may develop.
Horizontal spread of infection may track across the internal sphincter into the anal canal or in the opposite direction across the external sphincter into the ischiorectalfossa to form an ischiorectal abscess. The abscess may be large, especially if neglected or treated only with antibiotics and allowed to expand to the roof of the fossa or even through it into the supralevator space after traversing the levatorani muscle and downward to the perianal skin. The patient may complain of pain and fever before an erythematous mass is detectable. Ultimately, an obvious red, fluctuant mass is visible. The infectious process may spread circumferentially from one side to the other of the intersphincteric space, the supralevator space, or the ischiorectalfossa, producing the complex, horseshoe abscess.
Fistula in Ano • Anorectal sepsis can be complicated by a fistula in ano in about 25% of patients. Most fistulas derive from sepsis originating in the anal canal glands at the dentate line. The path of a fistula is determined by the local anatomy; most commonly, they track in the fascial or fatty planes, especially the intersphincteric space between the internal and the external sphincter into the ischiorectal fascia. In such instances, the track passes directly to the perineal skin. • In some cases, circumferential spread may also occur in the ischiorectalfossa, with the track passing from one fossa to the contralateral one through the posterior rectum, a fistula known as the horseshoe fistula.
Parks classification of Anorectal Fistulas • Fistulas usually fall under four main anatomic categories as described by Parks and colleagues in 1976. • Intersphincteric(the most common): The fistula track is confined to the intersphincteric plane. • Trans-sphincteric: The fistula connects the intersphincteric plane with the ischiorectalfossa by perforating the external sphincter. • Suprasphincteric: Similar to trans-sphincteric, but the track loops over the external sphincter and perforates the levatorani. • Extrasphincteric: The track passes from the rectum to perineal skin, completely external to the sphincteric complex. The track is completely outside the sphincteric apparatus. Causes typically include trauma, either external or internal (e.g., fish bone piercing one wall of rectum), carcinoma, or Crohn’s disease. Treatment is difficult, lengthy, and usually involves colostomy.
Presentation • Mucopurulent discharge • A fistula may first present as an acute abscess or, at times, simply as a draining sinus that may irritate the perineal skin. • On examination, subcutaneoinduration may be traced from the external opening to the anal canal. Digital examination may reveal a palpable nodule in the wall of the anal canal, an indication of the primary opening. A probe can be eased gently (not forcefully) from the external skin opening to the internal, anal canal opening.
Clinical assessment • A full medical (including obstetric, gastrointestinal, anal surgical and continence) history and proctosigmoidoscopy are necessary to gain information about sphincter strength and to exclude associated conditions. The key points to determine are the site of the internal opening; the site of the external opening(s); the course of the primary track; the presence of secondary extensions; and the presence of other conditions complicating the fistula. • Goodsall’s rule, used to indicate the likely position of the internal opening according to the position of the external opening(s), is helpful but not infallible. • The site of the internal opening may be felt as a point of induration or seen as an enlarged papilla. • Probing in an awake patient is painful, unhelpful and can be dangerous. • Full examination under anaesthesia should be repeated before surgical intervention. • Dilute hydrogen peroxide, instilled via the external opening, is a very useful way of demonstrating the site of the internal opening; gentle use of probes) and a finger in the anorectum usually delineates primary and secondary tracks and their relations to the sphincters. Any concerns about fistula topography at clinical examination or examination under anaesthesia (morecommon after previous unsuccessful surgery) should prompt further investigations before surgical intervention.
MRI or endorectal ultrasound may be helpful in difficult and persistent high fistulas .
Differential Diagnosis • • Inflammatory bowel disease (Crohn disease) • • Pilonidal disease • • Hidradenitis suppurativa • • Anal tuberculosis
Management of fistula in ano should include the following steps: Drainage of primary intersphincteric infection in all types of fistulas, as well as the primary track across the external phincter and secondary tracks within the anorectalfossa, is key. • For superficial fistulas involving small quantities of sphincter muscle, primary fistulotomyis simple and definitive. • For anterior fistulas in women and fistulas involving greater than one fourth to one half the bulk of sphincter muscles, seton placement should be preferred over primary fistulotomy . • In rare circumstances with complex, deep, or recurrent fistulas, newer alternatives to fistulotomy are preferred to avoid the complication of fecal incontinence. Fibrin glue injections of the track and advancement flap closure of the primary openings can heal 69% of complex fistulas. • For Suprasphinctericand Extrasphincteric:Treatment is difficult, lengthy, and usually involves colostomy
Close follow-up and careful nursing of the wound by a physician-nurse team involve Seitz baths and wound dressing to ensure healing from the depth of the wound to the surface. • A seton of monofilament nylon tied loosely around the fistulous track may be used to drain the transsphincteric track traveling above the anal valves for a suprasphincteric fistula.
Pilonidal Disease • The term pilonidal sinus describes a condition found in the natal cleft overlying the coccyx, consisting of one or more, usually noninfected, midline openings, which communicate with a fibrous track lined by granulation tissue and containing hair lying loosely within the lumen. • Pilonidal infections and chronic pilonidal sinuses typically occur in the midline of the sacrococcygeal skin of young men. Although the exact pathogenesis of pilonidal disease remains controversial, hair seems to play a central role in the process of infection • This is consistent with the clinical observation that pilonidal patients are often hirsute and that pilonidal diseases rarely occurs in populations with less body hair. • It is uncommon for pilonidal disease to be confused with clinical disorders such as anal fistulas, skin disorders, underlying malignancies, or true sacrococcygeal sinuses.
Presentation • Patients presenting acutely with new-onset disease may have a painful fluctuant abscess or a draining infected sinus. • Recurring sinus and infections.
Acute Management • Abscess can be drained using local anesthesia. • For both abscesses and sinuses, hair should be removed from the wound and local skin should be shaved weekly to prevent the reintroduction of hair. Laser depilation can also be used to accomplish long-lasting, but temporary, hair removal. • Ideally, these patients should be seen weekly in the office for wound care until there is complete healing.
Management of chronic PNS • For those patients who have recurring infections, more definitive operative management is warranted. Numerous procedures have been described in literature ranging from simple incision and drainage to complex plastic flaps for cleft obliteration.
Rectal Fixation, Abnormal • Attachment of the rectum to the sacrum has lengthened, allowing rectum to block defecation, protrude into the vagina, or prolapse through the anus. • Female to male ratio is 5:1 • 2 types of rectal prolapse A) Mucosal ( partial ) B) complete