Download
1 / 36
480 likes | 1.36k Vues
Steroid Hormones,Congenital Adrenal hyperplasia and Testicular Feminaization. Objectives . Overview of Steroids The Role of Cholesterol Adrenal Steroids Steroids from the Testis Ovarian Steroids Congenital Adrenal Hyperplas Testicular Feminization. Steroid hormones.

E N D
Steroid Hormones,Congenital Adrenal hyperplasia and Testicular Feminaization
Objectives Overview of Steroids The Role of Cholesterol Adrenal Steroids Steroids from the Testis Ovarian Steroids Congenital Adrenal Hyperplas Testicular Feminization
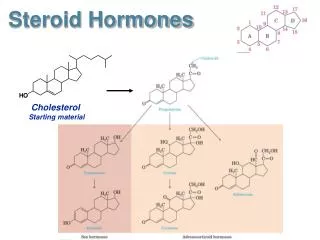
Steroid hormones • All steroid hormones are derived from cholesterol and differ only in the ring structure and side chains attached to it. • All steroid hormones are lipid soluble and thus are freely permeable to membranes so are not stored in cells
Steroid Hormones • produced in the adrenal cortex, testis, ovary, and some peripheral tissues (adipose tissue, the brain) • All steroid hormones share a typical (but not identical) ring structure.
Steroid hormones have to be carried in the blood complexed to specific binding globulins. • Corticosteroid binding globulin carries cortisol • Sex steroid binding globulin carries testosterone and estradiol • In some cases a steroid is secreted by one cell and is converted to the active steroid by the target cell:
Types of steroid hormones • Glucocorticoids; cortisol is the major representative in most mammals • Mineralocorticoids; aldosterone being most prominent • Androgens such as testosterone • Estrogens, including estradiol and estrone • Progestogens (also known a progestins) such as progesterone
Functions of Steroid Hormones • Steroid hormones play important roles in: - carbohydrate regulation (glucocorticoids) - mineral balance (mineralocorticoids) - reproductive functions (gonadal steroids) • Steroids also play roles in inflammatory responses, stress responses, bone metabolism, cardiovascular fitness, behavior, cognition, and mood.
Organization of the Adrenal Gland There is an adrenal cortex and adrenal medulla • The adrenal glands comprise 3 separate hormone systems: • The zonaglomerulosa: • secretes aldosterone • The zonafasciculata & reticularis: • secrete cortisol & the adrenal androgens • The adrenal medulla: • secretes adrenaline
Steroid hormone synthesis A series of enzymatic steps in the mitochondria and ER of steroidogenic tissues convert cholesterol into all of the other steroid hormones and intermediates. An important control point this process is the transport of free cholesterol from the cytoplasm into mitochondria. This step is carried out by the Steroidogenic Acute Regulatory Protein (StAR) im
Source of Cholesterol for Steroid Synthesis LH Extracellularlipoprotein Cholesterolpool acetate ATP cAMP cholesterol PKA+ Pregnenolone 3bHSD Progesterone P450c17 Androstenedione 17bHSD TESTOSTERONE
Adrenal Steroidogenesis • The first enzymatic step is the conversion of cholesterol to pregnenolone, which occurs in the mitochondria. • This reaction is carried out by the enzyme, cytochrome P450 side-chain cleavage (P450scc; also called desmolase, or CYP11A1). • This is a rate limiting, nonreversible step in the initiation of steroid biosynthesis. • This step occurs in adrenal, ovary, and testis.
Steroid Hormone Synthesis Cholesterol Pregnenolone (C21) 3-β-Hydroxysteroid dehydrogenase Progesterone (C21) 21-α-Hydroxylase 17-α-Hydroxylase 17-α-Hydroxyprogesterone (C21) 11-Deoxycorticosterone (C21) Androstenedione (C19) 11-Deoxycortisol (C21) 11- β-Hydroxylase Testosterone (C19) Peripheral tissues Corticosterone Aldosterone (C21) Cortisol (C21) Estradiol (C18)
Adrenal Steroidogenesis What determines which pathway is taken? • Each step of the pathway is regulated by a specific enzyme. • Different zones of the adrenal cortex have different relative activities of enzymes, resulting in different chemical reactions taking place. • These enzymes are located in the smooth ER.
Regulation of ACTH and Cortisol Secretion: 1. Negative feedback control: • ACTH release from the anterior pituitary is stimulated by hypothalamic secretion of corticotrophin releasing hormone (CRH). • CRH ACTH [Cortisol] • [Cortisol] or synthetic steroid suppress CRH & ACTH secretion Hypothalamus Pituitary Adrenal
Pathway of Testosterone Production in the Testis • The production of androgens from cholesterol is identical to that in the adrenal, except that it continues from androstenedione to testosterone. 17b-hydroxysteroid oxidoreductase androstenedione testosterone
Production of Steroids in the Testis • The main steroid produced in the male is testosterone, from the testis. . • In the male, there is peripheral conversion of testosterone to dihydrotestosterone (in androgen target tissues, like muscle) by 5a-reductase, • or to • and estradiol (mostly in adipose tissue) (E2) by cytochrome P450 aromatase.
Control of testicular function by the gonadotrophins Hypothalamus GnRH + - - Anterior Pituitary FSH LH + + Testis Testosterone Inhibin AR Peripheral tissue Spermatogenesis
OvarianSteroidogenesis • The ovary produces estrogens (primarily estradiol), progesterone, and androgens. • Ovarian steroids are secreted primarily from ovarian follicles and corpora lutea.
The Puzzle of Estrogen Production in the Ovary • In the ovary, estradiol is formed from the conversion of testosterone into estradiol by the enzyme cytochrome P450 aromatase. This occurs in granulosa cells. • However, granulosa cells do not have the enzyme 17a-hydroxylase/lyase, and thus cannot convert progesterone into androgens. • Where do the androgens required for estrogen production in granulosa cells come from?
LH FSH LH receptor cholesterol androgens estradiol aromatase androgens theca cell granulosa cell The Two-Cell Theory of Estrogen Production in the Ovary • Numerous studies have now shown that the androgens required for aromatization come from the neighboring theca cells:
Receptorswhich work with the same mechanism • Steroid hormones • Thyroid hormones • Retinoic acid • 1,25-dihydroxycholecalciferol All are members of a’”superfamily’” of structurally related gene regulators that function in a similar way
Congenital Adrenal Hyperplasia (CAH) • It is the result of an inherited enzyme defect in steroid biosynthesis • The adrenals : • Cannot secrete cortisol absent negative feedback to the pituitary) ACTH continues to drive steroid biosynthesis adrenal hyperplasia and accumulation of cortisol precursors (depending on which enzyme is lacking) • Cannot secrete aldosterone electrolyte disturbances • Hyponatraemia • Hyperkalaemia • The condition might be fatal unless diagnosed early
21 -Hydroxylase Deficiency 17-hydroxy-progesterone Progesterone Androstenedione X 21 -hydroxylase In peripheral tissues 11-deoxycorticosterone Testosterone Precocious sexual development in ♂ Virilisation of ♀
Congenital Adrenal Hyperplasia (CAH), 21 -Hydroxylase Deficiency • Autosomal recessive condition • Impairs synthesis of cortisol & aldosterone • Accounts for ~ 95% of all cases of CAH • [cortisol] ACTH secretion Adrenal gland hyperplasia • Some of the accumulated precursors are diverted to the biosynthesis of sex hormones signs of androgen excess: • In severe cases, mineralocorticoid deficiency is evident salt & H2O loss hypovolaemia & shock neonatal adrenal crisis • Late presentation (adult life) is possible in less severe cases
Diagnosis of the most common type (21-hydroxylase deficiency) is be finding plasma [17-hydroxyprogesterone] as early as 4 days after birth. • stimulation of adrenal androgen production virilization in baby girls, & precocious puberty in boys. • Partial enzyme defect late onset form menstrual irregularity & hirsutism in young females.
Diagnosis • Serum sample taken at least 2 days after birth (earlier samples may contain maternally derived 17-hydroxyprogesterone • Classic 21-hydroxylase deficiency is characterized by markedly elevated serum levels of 17-hydroxyprogesterone • Late-onset 21-hydroxylase deficiency may require corticotropin stimulation test: • inject a 0.125-mg or 0.25-mg bolus of corticotropin • measure base-line and stimulated levels of 17-hydroxyprogesterone. High level after stimulation is diagnostic ( 2x upper reference range)
Genetics of 21 -Hydroxylase Deficiency • Mutations in the CYP21 gene • DNA testing and detection of mutations can be helpful for prenatal diagnosis and confirmation of diagnosis
11 -Hydroxylase Deficiency leads to high concentrations of 11-deoxycortisol Leads to high levels of 11-deoxy-corticosterone with mineralocorticoid effect (salt and water retention) Suppresses renin/angiotensin system low renin hypertension Musculanization in females (FPH) and early virilization in males
Disorders of Male Sexual Differentiation • They are rare group of disorders • The defect may be in: • Testosterone production (impaired testosterone production) • Androgen receptors (inactive androgen receptors target tissues cannot respond to stimulation by circulating testosterone; e.g., Testicular feminization syndrome)
TesticularFeminizationSyndrome • 46,XY karyotype • X-linked recessive disorder • Androgen receptor resistance high testosterone blood level • In peripheral tissue, testosterone will be converted by aromatase into estradiol feminization • Patients have normal testes & produce normal amounts of müllerian-inhibiting factor (MIF), therefore, affected individuals do not have fallopian tubes, a uterus, or a proximal (upper) vagina.
Clinical Picture: • Complete androgen insensitivity syndrome (CAIS): female external genitalia with normal labia, clitoris, and vaginal introitus (MPH) • Partial androgen insensitivity syndrome (PAIS): mildly virilized female external genitalia (clitorimegaly without other external anomalies) to mildly undervirilized male external genitalia (hypospadias and/or diminished penile size)
Take Home Message:Steroid Hormones: Characteristics • Are made from cholesterol, are lipophilic & can enter target cell • Are immediately released from cell after synthesis • Interact with cytoplasmic or nuclear receptors • Activate DNA for protein synthesis • Are slower acting and have longer half-life than peptide hormones • Examples: cortisol, estrogen & testosterone