Download
1 / 1
10 likes | 110 Vues
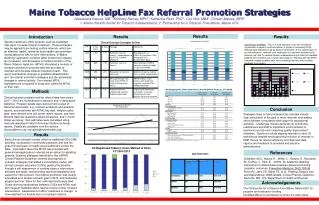
Maine Tobacco HelpLine Fax Referral Promotion Strategies Alessandra Kazura, MD 1 ; Kimberly Harvey, MPH 1 ; Katherine Ryan, PhD 1 ; Cori Holt, MBA 1 ; Dorean Maines, MPA 2 1. Maine1Health Center for Tobacco Independence; 2. Partnership for a Tobacco-Free Maine, Maine CDC. Results.

E N D
Maine Tobacco HelpLine Fax Referral Promotion Strategies Alessandra Kazura, MD1; Kimberly Harvey, MPH1; Katherine Ryan, PhD1; Cori Holt, MBA1; Dorean Maines, MPA2 1. Maine1Health Center for Tobacco Independence; 2. Partnership for a Tobacco-Free Maine, Maine CDC Results Insert your text here. Remember, the template is only to get you started, and can be changed to suit your unique needs Results Results Introduction Insert your text here. Remember, the template is only to get you started, and can be changed to suit your unique nee Specific healthcare office systems, such as expanded vital signs, increase tobacco treatment. These strategies may be applied to promoting quitline referrals, which are an effective “assist” option for busy health care providers incorporating the 5As for brief interventions. In Maine, declining registration numbers (after boosts from tobacco tax increases), and decreases in media promotion of the Maine Tobacco HelpLine (MTHL) stimulated a revision of outreach activities to promote referrals as a way to maintain and increase tobacco treatment reach. This report summarizes changes in guideline dissemination and fax referral promotion strategies and the associated changes in referral activity. Fax referred MTHL registrants are compared to those who called the MTHL on their own. Clinical Outreach Strategies by Year Case Study: InterMed. This is a multi-specialty, multi-site healthcare organization located in southern Maine. A target of increasing MTHL referrals was endorsed in as an explicit component of the system goal “to provide education, referrals, and medication for long term abstinence for tobacco use” and “to assess tobacco independence quit rates for InterMed patients who currently use or have used tobacco.” Working with the MTHL, Intermed created a patient path and is tracking referrals and providing feedback to providers. Methods Clinical outreach program and fax referral data from years 2007 –2012 are summarized in narrative and in descriptive statistics. Program details were derived from review of historical documents, e.g. contract workplans and quarterly reports, and interviews with MTHL key staff. Helpline caller data were derived from call center metric reports, and from Minimal Data Set questions asked at baseline and 7-month follow-up survey. Quit estimates were calculated using methods described in North American Quitline technical reports. Details are available from the authors (kazura@mmc.org; harveyk2@mainehealth.org). Conclusion Strategies likely to have increased fax referrals include clear articulation of the goal of more referrals, and adding office systems consultation and support to educational activities. Challenges include demands on community practitioners and staff to implement a full transition to electronic records and competing quality improvement initiatives. Solutions include aligning referrals to other QI activities as feasible and supporting inclusion of referrals in EMR menus for referral efficiency and improved data capture and feedback to providers and practice administrators. Results Early clinical outreach models relied on traditional CEU/CME activities, conducted in community practices, and had the goal of broad reach of health care practitioners across the state. Information about the MTHL was provided with general messaging about referrals as an option for assisting patients. Systems strategies described in the USPHS Clinical Practice Guideline informed development of outreach strategies that added a consultation model, with clinical outreach educators (COEs) guiding the practice through a self-assessment of existing tobacco intervention activities and goals, and providing technical assistance and support for improvement. Fax referral promotion was clearly articulated as a clinical outreach goal in 2010, and marketing slogans such as “strive for five” referrals/month were tried. Closer working relationships between COEs and MTHL staff, with frequent feedback about referral volume further focused interventions. Assessment of office “readiness to change” is now matched to a flexible menu of outreach options. All Registered Tobacco Users Method of Entry CY 2007-2012 References Quit Outcomes Goldstein, M.G., Niaura, R., Willey, C., Kazura, A., Rakowski, W., DePue, J., Park, E. (2003). An academic detailing intervention to disseminate physician-delivered smoking cessation outcomes. Preventive Medicine, 36(2):185-96. Fiore MC, Jaen CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service. May 2008. Acknowledgements The Partnership for a Tobacco-Free Maine, Maine CDC for program and evaluation funding. InterMed Maine for permission to share the case study.