PROGRESS NOTE (SOAP Notes)
PROGRESS NOTE (SOAP Notes). H.A.Soleimani MD Gastroenterologist. PROGRESS NOTE (SOAP Notes (. The medical student should be the person most intimately aware of the patient's status, it is appropriate that he or she be given the responsibility of writing the note each day.


PROGRESS NOTE (SOAP Notes)
E N D
Presentation Transcript
PROGRESS NOTE(SOAP Notes) H.A.Soleimani MD Gastroenterologist
PROGRESS NOTE (SOAP Notes ( • The medical studentshould be the person most intimately aware of the patient's status, it is appropriate that he or shebe given the responsibility of writing the note each day.
PROGRESS NOTE (SOAP Notes ( • One of the most important documents in the medical record is the daily progress note
PROGRESS NOTE (SOAP Notes ( The progress note • Reflect what transpired during the previous 24hours • Updates a patient's clinical course each day • Summarizes the ward team's ongoing assessmentand plan.
PROGRESS NOTE (SOAP Notes ( • Progressnote include a directed or focal examination, and plans for further evaluation.
Subjective Objective Assessment Plan S=Subjective Use the SOAP format O=Objective A=Assessment P=Plan
Progress note • Uses: 1,Daily evaluation of a hospitalized patient 2,Return visit in outpatient clinic
Progress note • Subjective (Focused history) 1. Information you have learned from the patient or people caring for the patient
SUBJECTIVE SUMMARY • Thenote begins with a statement of the patient's own (subjective) assessment of his condition.
SUBJECTIVE SUMMARY • The subjective portion should include some of the patient’s or parents' own words.
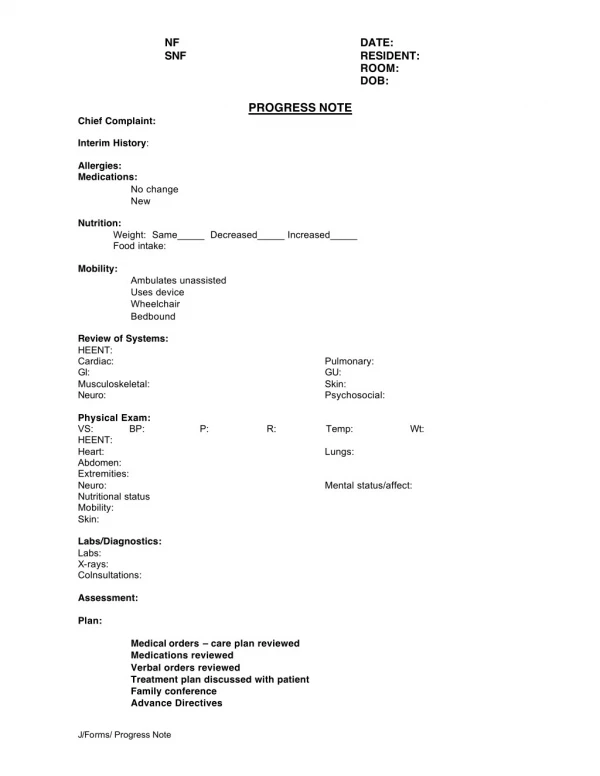
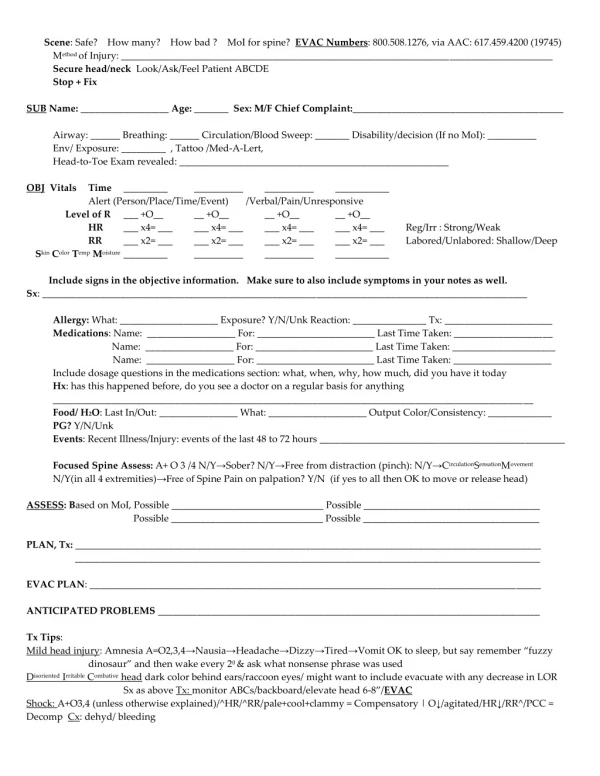
OBJECTIVE SUMMARY • 1 -Vital signs • 2-The patient's general appearance • 3-Physical exam findings • 4- Any diagnostic test results (Laboratory and imaging..)
OBJECTIVE SUMMARY VITAL SIGNS • Blood Presure • Pulse Rate • Respiration Rate • Temperature • (Weight, Pain, xygen Saturation? )
OBJECTIVE SUMMARY • The patient's general appearance should be noted after vital signs.
OBJECTIVE SUMMARY • PHYSICAL FINDINGS: An directed physical examination should be recorded with all pertinent areas described.
OBJECTIVE SUMMARY • Laboratory data: Although one will often wish to mention certain laboratory data in the assessment, there is noneed to list all of the results.
PROGRESS NOTE (SOAP Notes ( • Because the progress note is focused on "progress,' the assessment and plan section includesonly problems that are being addressed during the hospitalization.
ASSESSMENT • Assessment:Provide your working diagnosis and mention the state of the patient
ASSESSMENT • Identify the major or primary assessment supported by the patient database and any other associated assessments.
ASSESSMENT • 1.What do you feel is the patient’s differential diagnosis and why? • 2.Organized by problem or organ system
ASSESSMENT • Every day problem list with Every day differential diagnosis for each problem
PLAN • A separate plan should be developed for each assessment.
PLAN • Each plan should be divided into 1.Diagnostics(Lab .x.ray..) 2.Therapeutic 3.Patient Education 4.Health Promotion Strategies
PLAN For each problem what diagnostic testing will you order? How will you treat each problem or diseases?
PLAN Action planned for each problem A&P( assessment and plan)
PROGRESS NOTE (SOAP Notes ( • Progress note maybe quite brief. It does not need to be crafted in fallsentences as long as it is easily comprehensible.
PROGRESS NOTE (SOAP Notes ( • It is also important to remember that the progress note, like the oral and written presentations, is partof the student's education and should be reviewed with the intern, resident, or attending.
PROGRESS NOTE (SOAP Notes ( • The date, time, title, are essential • USE BLACK INK • SIGN AND write YOUR NAME on any chart notes
EXAMPLE OF PROGRESS NOTE (SOAP Notes)
EXAMPLE OF PROGRESS NOTE SUBJECTIVE SUBJECTIVE SUBJECTIVE
PROGRESS NOTE (SOAP Notes Mr. Hamedi is an 84 year old man who comes to the hospital 7 day ago for angiography and today he have worsening leg swelling. The swelling started 3 days ago in his ankles and has progressively moved toward his groin.
PROGRESS NOTE (SOAP Notes • He also feels short of breath. For the past two days he can’t walk without resting halfway. He has difficulty breathing when lying in bed.
EXAMPLE OF PROGRESS NOTE OBJECTIVE OBJECTIVE OBJECTIVE
PROGRESS NOTE (SOAP Notes) • 1. Vital signs: BP 120/72, HR 68, RR 20, T 36 • 2. Chest: crackles 1/3 up bilaterally.
PROGRESS NOTE (SOAP Notes) • Extremities: No erythema or tenderness. 2+ pitting edema bilaterally to his knees.
PROGRESS NOTE (SOAP Notes) • 3.Cardiac: Regular rate and rhythm, normal S1 and S2, S3 is present, No murmur
PROGRESS NOTE (SOAP Notes) • Abdomen: Normoactive bowel sounds, soft, non-tender, non-distended, no hepatomegaly or splenomegaly
PROGRESS NOTE (SOAP Notes) • Labs visit: Sodium 125 (135 -145) Potassium 3.6(3.5 – 5.1) BUN 40 (10 – 20) Creatinine1.5 (0.6 – 1.3)
EXAMPLE OF PROGRESS NOTE ASSESSMENT ASSESSMENT ASSESSMENT
PROGRESS NOTE (SOAP Notes) Problem • Shortness of Breath • New dyspnea on exertion • S3 crackles and edema ASSESSMENT 1.Congestive heart failureor new angina
PROGRESS NOTE (SOAP Notes) Problem Edema ASSESSMENT 1.Congestive heart failureor new angina 2.Nephrotic syndrome 3.hypothyroidism
PROGRESS NOTE (SOAP Notes) No suggestion of pure pulmonary disease No suggestion of Hypertension –Blood presure is well controlled and is probably not contributing to his presenting complaints.
EXAMPLE OF PROGRESS NOTE PLAN PLAN PLAN
Congestive heart failureor new angina • We will order an EKG right now to assess cardiac rhythm and acute injury.
Congestive heart failureor new angina • We will also send him for an echocardiogram to measure his cardiac function.
Nephrotic syndrome • We will check a urinalysis to rule out the proteinuria of nephrotic syndrome
Hypothyroidism • Check a thyroid stimulating hormone level to evaluate his thyroid function.
Hypertension • No changes are needed in his blood pressure medication.