Download
1 / 40
400 likes | 579 Vues
Paediatric Burns- fluids and the airway. Dr FA Potter Alder Hey Hospital. About 6000 children admitted to hospital with thermal injuries each year 120 major burns each year A real problem but not common occurrence for any one hospital. The Airway.

E N D
Paediatric Burns- fluids and the airway Dr FA Potter Alder Hey Hospital
About 6000 children admitted to hospital with thermal injuries each year • 120 major burns each year • A real problem but not common occurrence for any one hospital
The Airway • Loss of Control through decreased level of consciousness • Impending closure of the airway from burn associated swelling • Treatment of respiratory failure • Inhalational injury • ARDS • Fluid resuscitation • Humanitarian/Practical Considerations
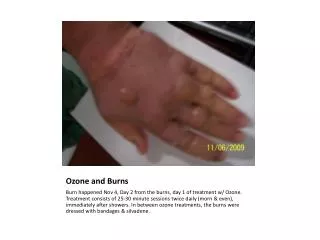
Burn Shock - local • Dead tissue • Ischaemic zone • Inflammation-histamine, prostaglandin,thromboxane,NO • local oedema • Reactive Oxygen Species further local damage;further inflammation
Burn Shock –systemic 1 • TNFalpha, interleukin-1,2,5,8 interferon gamma • SIRS • Increased microvascular permeability • Vasodilatation • Decreased cardiac contractility • Intravascular fluid, electrolytes,proteininterstitial • Lymph vessel obstruction (platelets, leukocytes) • Generalised oedema 24-48hr
Burn Shock –systemic 2 • Loss of intravascular volume to interstitium • Increased evaporative loss through burn wound • Decreased preload • Decreased cardiac contractility • Decreased cardiac output • Decreased end organ perfusion • MULTIPLE ORGAN FAILURE • FLUID RESUSCITATION
What Fluid ? • Eggnog (& enemas) Fauntleroy 1919 • Plasma Harkins 1942 (fluid relate to area of burn) • Albumin Evan’s formula 1952 • 1ml/kg/%burn NS +1ml/kg/%burn albumin +2000ml glucose. Second 24hr: half the saline +albumin +glucose • Crystalloid Baxter & Shires 1968
Estimation of Burn Area Burn extent Rule of Nines Lund and Browder charts Patient weight Calculation using formula
Parkland 4ml/kg/%burn Hartmann’s solution Half over 8hr Half over 16hr + maintenance Mount Vernon O.5ml/kg/%burn Plasma 6 periods 4hr 8hr 12hr 18hr 24hr 36hr post burn + maintenance How Much?
Albumin • Meta-analysis questioning use of albumin in critically ill patients • 1998-2004 • ‘ If I survived, I would attempt to sue anyone who had given me an infusion of albumin, and I would not give my informed consent to take part in a randomised trial’ • Burns +others
Where are we now?RHJ Baker MA Akhavani,N Jallali. Journal of Plastic & Reconstructive Surgery 2007;60:682-685 • 78% UK units use Parkland • 11% Mount Vernon • 11% both • 75% paeds units Hartmann’s • 10% use albumin, 15% both • 50% do not change fluid after 24 hr
‘Fluid Creep’ • Tendency to give more fluid than Parkland dictates • 60% patients get more [J Burn Care Rehab 2000;21:91-5] • 7ml/kg/%burn [ J Burn Care Rehab 2002;23:258-65] • Surviving Sepsis Campaign 2004 – • Lactate, BE, central venous saturations. • Pulmonary Oedema, Abdominal Compartment Syndrome
Back to the future? • First 24 hrs • 4ml LR/kg/%burn + maintenance Second 24hrs 0.3-0.5 ml plasma over 8hr + dextrose / water to maintain urine output 98% of 516 children successfully resuscitated CR Baxter. Surgical Clinics of North America 1978;58:1313-22
Where might we go? • Haifa Formula • 1.5ml/kg/%burn FFP + 1ml/kg/%burn RL • + more RL if urine <0.5ml/kg/hr • 8%mortality (80% >80%burn) • Starches – if problems of coagulation solved
Inhalational Injury • Direct Burn – actual thermal injury supraglottic ;unless steam involved • Inhaled Gases- aldehydes,NO, NO2, SO2, PVC, CO • Inhaled Particulates • ALI From SIRS From Fluid Overload
CO affinity for Hb 200x that of oxygen Moves oxyhaemoglobin dissociation curve to left 10-30% headache 50% coma 70% fatal Half-life 4hr (air) 30-60min (high O2) Low CO often underestimates degree of injury Carbon Monoxide
Oedema of tracheobronchial mucosa Separation of epithelium Bronchial casts Parenchyma-congestion, oedema ,neutrophil Infiltration, hyaline membranes Bronchoscopy- diagnosis removal casts Xenon scanning CXR infiltrates over 5-10days Inhalational injury
TL Palmieri, P Warner et al. Journal of Burn Care & Research.2009 30;1:206-208 • 850 children 4 tertiary US centres over 10yr • 603 bronchoscopic findings • 216 clinical findings • 31 CO elevation • 710 survivors 140 non-survivors • TBSA burn 45% TBSA burn 70% • Cause of death 50 pulmonary, 31 sepsis, 15MOF 8burn shock
Management Shriners Hospital, Galveston TX • O2 maintain SpO2 >90% • Artificial cough 2hrly • Chest physio 4hrly • Nebulised N-Acetyl cysteine 4hrly • Nebulised heparin 4hrly • Sputum culture 3x week • TV 6ml/kg, PIP<35, permissive hypercapnoea
Intubation • Window • Drugs • Devices • Fixation • Definitive
Drugs • Intravenous Induction • Suxamethonium • Rapid sequence • Inhalational Induction • Sevoflurane in oxygen
Fixation • Difficult • Oedema displacement of tube • Tying, stapling, wiring to teeth
Tracheostomy -anti • 16 patients more than 55% burn vs • 9 patients with tracheostomy • Pulmonary sepsis 78% trache group • Pulmonary culture=burn wound culture • Avoid if at all possible • FE Eckhauser J Billotte JF Burke WC Quimby • American Journal of Surgery 1974; 127:418-23
Tracheostomy-pro • 1549 pediatric burn patients <4yrs old • 180 intubated • 76 tracheostomy (20-31-18-7) • 20 tracheostomies done through eschar • No loss of airway • 7 children had problems decannulating (3 had severe inhalational injury) • 45/76 pneumonia vs 28/104 • But no patient deteriorated because of tracheostomy • CE Coln, GF Purdue,JL Hunt. Archives of Surgery 1998;1333:537-40
Conclusions • Early management of the airway is crucial • Early Fluid resuscitation should follow a formula • Later fluid management is more controversial • Centralisation may give more answers