Download
1 / 50
510 likes | 746 Vues
Airway and Oxygen. System Orientation. Objectives. Breathing Respiratory Anatomy Assessment Rescue breathing Airway obstruction Oxygen delivery devices Suction. Breathing. Why we breathe To bring oxygen into the body To expel carbon dioxide from the body Breathing is automatic.

E N D
Airway and Oxygen System Orientation
Objectives • Breathing • Respiratory Anatomy • Assessment • Rescue breathing • Airway obstruction • Oxygen delivery devices • Suction
Breathing • Why we breathe • To bring oxygen into the body • To expel carbon dioxide from the body • Breathing is automatic
Clinical Death—The moment the breathing and heartbeat stop Brain Damage—within 4–6 minutes Biological Death—within 10 minutes
Breathing • How We Breathe: • Inspiration: • Rib and diaphragm muscles contract. • Chest cavity expands. • The volume inside each lung increases. • The pressure inside each lung decreases. • When the pressure inside the lungs becomes less than the pressure in the atmosphere, air rushes into the lungs.
Breathing • How We Breathe: • Inspiration is an active process. • Expiration is a passive process.
Assessment • Signs of Normal Breathing: • Look for rise and fall of the chest. • Listen for air moving: • The sounds should be quiet like a soft breeze. • No unusual sounds • Feel for air moving. • Observe skin color: • Should not be pale or ashen • Should not be tinted blue or gray • Look at the lips, eyes, and nail beds
Assessment • Signs of Inadequate Breathing: • No chest movements, or uneven chest movements • No air heard or felt at the nose or mouth • Noisy breathing or gasping sounds • Breathing that is irregular, too rapid, or too slow • Breathing that is too shallow, or deep and labored
Assessment • Signs of Inadequate Breathing: • Breathing that uses muscles in the upper chest and around the neck • Nostrils that flare when breathing, especially in children • Skin that is tinted blue, gray, or ashen • Sitting or leaning forward in a tripod position
Normal Respiratory Rates • Respirations: • The normal respiratory rate for adults is 12–20 breaths per minute. • > 28 or < 8 are considered serious. • Newborn infants = 25–50 breaths per min. • Up to 5 years old = 20–30 breaths per min. • 5 to 12 years of age = 15–30 breaths per min.
Opening The Airway • Repositioning the Head: • The head-tilt, chin-lift maneuver, is used for ill or injured patients with no possibility of spinal injury. • Used when no c-spine injury is suspected • The jaw-thrust maneuver, is used for patients who have a mechanism of injury that indicates possible spinal injury. • Used for those who have a suspected c-spine injury or in those who are unresponsive with mechanism of injury in which trauma is suspected
Airway Obstruction • Causes of Airway Obstruction
Airway Obstruction • Causes • Tongue • Epiglottis • Foreign objects
Airway Obstruction • Signs • Snoring • Gurgling • Crowing • Stridor • Cyanosis • Anxiety • Labored breathing • Inability to speak
Rescue Breathing • Use personal protective equipment and barrier devices. • One example of a barrier device is the pocketface mask.
Mouth to Mask • Most effective technique • Can be used with airway adjuncts
Mouth to Mask • Problems • Failure to maintain a tight seal • Failure to tilt the head back to open the airway • Failure to deliver enough breath to see the chest rise • Providing breaths too quickly • Failure to recognize airway obstruction
Bag-Valve-Mask (BVM) Ventilator Pediatric and adult BVM ventilators
Bag-Valve-Mask (BVM) Ventilator Hand positioning for using the BVM with a single rescuer
Aids to Resuscitation • Oropharyngeal Airways
Aids to Resuscitation • Select Oropharyngeal Airway
Aids to Resuscitation • Another Way to Measure
Aids to Resuscitation • Nasopharyngeal Airway
Aids to Resuscitation • Determine Proper Size
Aids to Resuscitation • Gently Advance Airway
Suction Systems • Suctioning Techniques: • USE PERSONAL PROTECTIVE EQUIPMENT. • Never suction for longer than 15 seconds at a time. • Measure the tip of the catheter from the patient’s earlobe to the corner of the mouth. • Suction only as you remove the tip or catheter. • REMAIN ALERT FOR THE PATIENT’S GAG REFLEX AND FOR SIGNS OF VOMITING.
Suction Systems • Oxygen-powered suction unit • Electrically-powered suction unit • Portable hand-operated suction unit • Portable electrical suction unit
Suction Systems • Positioning a Rigid Pharyngeal (Throat) Tip
First Responder’s Role • Dependent on local protocols: • May require direct orders • May be written as a standing order • Do only what you have been trained to do. • Basic life support is possible without equipment. • If you are allowed to use equipment, you must maintain it and train with it.
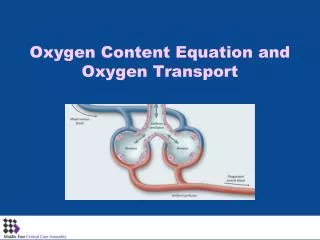
Oxygen Therapy • Equipment for Oxygen Therapy: • Oxygen cylinder • Pressure regulator • Flowmeter • Delivery device
Oxygen Therapy An oxygen delivery system
Oxygen Therapy Nasal cannula properly placed
Oxygen Therapy Non-rebreather mask
You are called for a 20 year-old male patient, struck by a car. You find the patient unresponsive. You do not see the patient’s chest rise when he breathes, but you hear gurgling from his airway. What airway control measures might you take for this patient? Check Your Understanding
Summary • Breathing • Respiratory Anatomy • Assessment • Rescue Breathing • Airway Obstruction • Aids to Resuscitation • Suction Systems
“Hearts and Brains are going to die” Peter Safar MD EMS has the most opportunity to perform CPR, so we should be good at performing good, quality CPR CPR/AED
CPR/AED • Why is CPR Important • Studies have shown that the general population will start CPR only 1/3 of the time and only 15% of that total is done correctly
CPR/AED • Lets look at the basics: • The first step is to determine responsiveness, if no response open the airway, check for breathing, and determine if a pulse is present
CPR/AED • Not Breathing and No Pulse: • Give 2 breaths-enough to see the chest rise • Give 30 chest compressions-allow for chest recoil between compressions • Give 5 cycles of 30:2 before rechecking a pulse
CPR/AED • Chest compressions and breaths are the same for adults, child, and infant • Adult age starts at the onset of puberty (12-14 yoa) • Child is age 1 – onset of puberty • Infant is anyone under the age of 1, chest compressions are delivered using 2 fingers, and remember a full head tilt should not be given as you may obstruct the airway
CPR/AED • The AED should be applied as soon as possible to the patients bare chest • Make sure the pads adhere to the skin • Remove all clothing from the area where the pads need to be placed • Remove any medication patches from the area • Shave any chest hair, the pads need to be on as much bare skin as possible • If the patient has an implanted Pacemaker, place the pad at least an inch away
CPR/AED • AEDs are set to correct the cardiac arrhythmias of V-Fib and V-Tach
CPR/AED • While there are many styles of AEDs they all work the same. The first step is to turn the unit on and follow the voice prompts.
CPR/AED • There are some safety considerations with the AED and Children: • If the unit has child pads use these on children between the ages of 1-8. • Never use child pads on an adult, the energy delivered by child pads is not enough for an adult, since the child pads reduce the energy from 200J to 50J • AEDs should not be used on infants