Download

1 / 36
360 likes | 572 Vues
Delivering value for your money NOVEMBER 2013. This presentation will cover…. How much we know about the state of safety and quality in the Australian healthcare system How safe are our hospitals and health services The purpose of the National Safety and Quality Health Service Standards

E N D
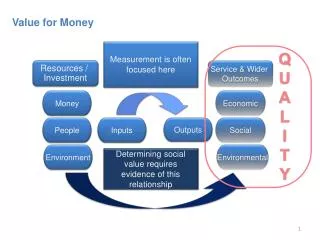
Delivering value for your money NOVEMBER 2013
This presentation will cover… • How much we know about the state of safety and quality in the Australian healthcare system • How safe are our hospitals and health services • The purpose of the National Safety and Quality Health Service Standards • Using medical practice variation to improve quality
Safety and Quality • Safety • Protect the patient from harm • Quality • Appropriateness • Effectiveness People + Systems
The Australian Health Care System The Australian health system is consistently one of the top performers in OECD countries 7th longest life expectancy at birth life expectancy at birth 82 yrs Top 5 countries for survival after heart attack & cancer Spectacular” declines in death from CVD (Australia’s Health) 8.9% GDP compared with OECD average 9.3%
Do the sick no harm “It may seem a strange principle to enunciate as the very first requirement in a Hospital that it should do the sick no harm.” Nightingale, F. First sentence of Preface to Notes on Hospitals (1859, 3rd. Ed.,1863)
Patient harm • Around 12% adverse event rate • Estimated that 50% of these events are avoidable • Don’t know about the degree of harm • One in 300 chance of being harmed – compared with one in one million as aircraft traveller • Medication error • Patient falls • HAI • Deterioration and failure to respond • Suicide
Leadership • How safe are our hospitals and health services?
How do we assess safety? • Are patients/carers at the center of care? • How many patient complaints are received? Week/month/year • Are they resolved? • How many SAC1 & SAC2 events? • What is the HSMR? • What is the infection rate? • What is the hand washing rate? • What is the surgical mortality? • Results of latest climate survey? • How are staff assessed? • How are new technologies assessed?
Funders – Safety & Quality • Are you getting only good news? • Do you think that your providers are performing better than then they really are? • Do reports contain the concerning news as well as the good news? • What is world class performance and how do your providers compare? • Are metrics kept simple and meaningful? • Are these data shared with fund holders, patients and staff? • Where does the patient/carer story fit with your Board and Executive?
National Safety & Quality Health Service Standards • To protect the public from harm • To improve the quality of health service provision
NSQHS Standards Standard 2 Partnering with Consumers Standard 1 Governance for Safety and Quality in Health Service Organisations Standard 3 Healthcare Associated Infections Standard 10 Preventing Falls and Harm from Falls Standard 4 Medication Safety Standard 9 Recognising and Responding to Clinical Deterioration in Acute Health Care Standard 5 Patient Identification and Procedure Matching Standard 8 Preventing and Managing Pressure Injuries Standard 7 Blood and Blood Products Standard 6 Clinical Handover
The NSQHS Standards Standards 1 and 2 are overarching Standards 3 – 10 are clinical standards, selected because they address areas where: The impact of poor safety or quality of care is across a large patient population There is a known gap between existing delivery of care and best practice Improvement strategies exist that are evidence based and achievable
Update of outcomes end of November 2013 • 1320 public and private health services to be assessed over 3 years • 297 health public (57%) and private health (43%) services have undergone accreditation • Nationally • 51% have had accreditation status confirmed • 49% have actions that need to be addressed within 120 days
What is Medical Practice Variation? (MPV) • MPV across & within countries widely documented • The fact that MPV are not always linked to clinical needs or patient preference now common knowledge • Australian Atlas of Medical Practice Variation to identify anomalies • To stimulate change to bring practice back toward evidence • Decision support tools
Understanding Medical Practice Variation (MPV) • Effective Care: • Evidence based interventions for which the benefit exceeds the harms so that most pts should receive the services (immunisations or beta-blockers following heart attack) • Preference-sensitive care: • Treatment options exist but carry different benefits and risks (PSA screening vs. biopsy) • Lower-value care includes health care activities whose effectiveness has not been demonstrated • Plain x-ray for lower back pain, IVF treatment over 40
Unwarranted variation in care Underuse of effective care e.g. screening of diabetics for retinal disease, prophylaxis for VTE, chronic heart failure management Overuse of supply sensitive care e.g. overuse of acute care sector because of lack of infrastructure support for chronic disease in the community Misuse of preference sensitive care e.g. Failure to accurately communicate risks & benefits of alternative treatments & failure to base the choice of treatment on the patients values & preferences
Overuse More health care can lead to worse outcomes Almost all interventions have some risks of harm &/or side effects Intervention “creep” to different populations where benefit unproven or < harms Some services become widely used but are of little proven benefit
Overuse – lower back pain Routine imaging in low back pain < 6/52 duration Low back pain lifetime incidence of 80% In Australia 28% of patients with low back pain have X-Rays (US 42% of patients) Lumbar imaging for low back pain without indications of serious underlying conditions does not improve clinical outcomes Potential harms: unneeded follow up tests for incidental findings, irradiation exposure, increased risk of surgery & medical costs
Preference sensitive care Early stage prostate cancer Watchful waiting: many prostate cancers never progress to affect quality of life or survival, but some do Radiation: shrinks or eliminates cancer in the prostate, but there are risks of side effects Radical prostatectomy: removes prostate cancer entirely, but there are substantial risks of incontinence & impotence The Dartmouth Atlas of Health Care www.dartmouthatlas.org
Estimated Cost of Waste in US Health Care Failures of care delivery - $102-154 billion Failures of care coordination - $25-45 billion Overtreatment - $158-226 billion Administrative complexity - $107-389 billion Pricing failures - $84-178 billion Fraud & abuse - $82-272 billion Sum of midpoint estimates: $910 billion (34% of national health expenditures) Berwick & Hackbarth JAMA 2012
Preference sensitive care Studies show major gaps in people’s understanding of their treatment options Importance of outcomes, side effects, risks differ for individuals Patient preferences may be poorly understood by doctors – e.g. breast cancer Decisions tend to be driven by doctors & favour intervention Better informed patients often choose different treatments
IOM (Institute of Medicine). 2012. Best care at lower cost: The path to continuously learning health care in America.
Preference sensitive care Decision aids (booklets, videos, web tools) prepare people to participate in decisions that involve weighing potential benefits, risks & scientific uncertainties about interventions present sufficient information about options to help people clarify how they value benefits vs harms & what matters most allow informed judgments about options
Decision Aids Cochrane systematic review People using evidence-based decision aids had improved knowledge of options more accurate expectations of possible benefits & harms choices more consistent with informed values greater participation in decision making reduced choice of major elective surgery in favour of conservative options Stacey et al, 2011
IOM (Institute of Medicine). 2012. Best care at lower cost: The path to continuously learning health care in America.
OECD Medical Practice Variations • 2013 study – 14 countries • Key findings: • Little variation in low-risk and high benefit procedures (surgery after hip fracture) • More in country variation preference sensitive care (cardiac procedures and diagnostic tests) • Social health insurance based countries report relatively lower variation than tax-based health care systems • Australia stands out for revascularisation and knee interventions
CABG by Medicare Local, age and sex standardised number per 100,000 population
Knee arthroscopy by Medicare Local, age and sex standardised number per 100,000 population
Hysterectomy rates by Medicare Local and age-standardised number per 1,000 female population
Age-standardised rates of caesarian sections per 1000 live births