Download
1 / 41
410 likes | 437 Vues
This presentation discusses Ontario's approach to managing physicians who may be incapacitated and provides insights into the Physician Health Program. It also covers the evaluation of aging physicians and the perspectives on mandatory reporting and ethical obligations.

E N D
CONFRONTING THE CHALLENGES OF PHYSICIAN FITNESS FOR DUTYONTARIO EXPERIENCE Dr Michael Szul 416-967-2600 x299 mszul@cpso.on.ca COALITION FOR PHYSICIAN ENHANCEMENT Chicago June 2015 College of Physicians and Surgeons of Ontario QUALITY PROFESSIONALS | HEALTHY SYSTEM | PUBLIC TRUST
EDUCATIONAL OBJECTIVES: • Audience will understand Ontario’s: • Approach to managing physicians who may be incapacitated • Relationship to Physician Health Program of the Ontario Medical Association • Approach to MDs with Blood Borne Pathogens who do EPPs • Approach to assessing ageing MDs • Perspective re: Mandatory reporting and ethical reporting obligations
ROLE OF THE COLLEGERegulated Health Professions Act (RHPA) • Objects • To regulate…. • To develop • Standards of qualifications…. • Standards of practice…. • Standards of knowledge and skill…. • Professional ethics…. • To promote • Continuing evaluation, competence and improvement…. • Inter-professional collaboration…. • To administer the Health Professions Act… • Advertising, professional misconduct, registration, conflict of interest regulations • “…duty to serve and to protect the public interest”
WHAT INTERFERES WITH FITNESS? • Drugs • Mental Illness • Physical Illness • Blood-Borne Pathogens
SOURCES OF INFORMATION • Third party – 51% (not mandatory) • Pharmacists - information • Family members – concerns • Colleagues • Police • Institutional, facility or other mandatory reporting – 24% • Chief of Staff - Hospitals • Facility Directors - Health Facilities • Patient complaints – 15% • Self disclosure – 10% • Annual application • Phone calls to our Physician Advisory Service
DEFINITION OF “INCAPACITATED” ie (NOT FIT) • “Incapacitated” means…the member is suffering from a physical or mental condition or disorder that makes it desirable in the interest of the public that the member’s practice be subject to terms, conditions or limitations, or that the member be no longer permitted to practise – Regulated Health Professions Act
FOCUS OF FITNESS ASSESSMENTS • Substance abuse/dependency issues • Mental health issues - depression • Neurologic decline: • Dementia • Strokes • Parkinson’s • Visual • Head injury from MVAs • BBP
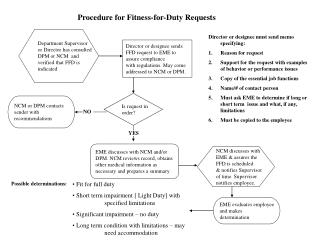
PROCESS • Notification/visit • Advice to contact Canadian Medical Protective Association • If substance misuse/mental health issue, info re: Physician Health Program (PHP) • Assessment by experts or accept undertaking to sign diagnostic/monitoring contract with Physician Health Program
PROCESS - 2 • Review and decision by committee of MDs and public members • Due process – right of response • If disagreement and risk of harm, hearing • Right of appeal • Most result in undertakings • To seek treatment where possible and to be monitored • To restrict practice, if a risk
ASSESSMENT TOOLS • If member does not sign diagnostic/monitoring contract with Physician Health Program, how do we assess health? • Documentary review • Medical records of FP, consultants • Hospital records • Interview • Psychiatrists • Addictions specialists • Neuropsychologists • Geriatricians • Neurologists • Multidisciplinary team • Expert panel for Blood Borne Pathogens (BP) if any doubt (MD’s identity anonymized unless hearing) • Requirement to cooperate – committee can suspend if lack of cooperation
ASSESSMENTS • Pilot- using single-source, multi-disciplinary setting, “Work, Stress and Health Program” at Centre for Addictions and Mental Health at University of Toronto • Faster, more convenient, too soon to evaluate its ultimate role • Ontario Telemedicine Network to allow certain assessments to be conducted remotely (accepted in principle - not yet done)
FAQ • Do all cases of serious mental or physical illness come to the attention of the College? • Risk of harm • Protection of the public • Do MDs have to report to the College any illness where they go on a leave of absence? • Re-entering Practice Policy • <6 m in 5 years • Not practising at all for 3 years
INCAPACITY INVESTIGATION • Goal is protection of the public • Negotiation • May result in some practice restriction until safe to practise • May result in supervision • With substance use and/or psychiatric issues, Physician Health Program (PHP) contracts are encouraged/accepted • If negotiation is not acceptable, there may be referral to Fitness to Practise Committee
INCAPACITY INVESTIGATIONS • In 2013, 64 new incapacity investigations • 7 referrals to Fitness to Practise • Most are resolved through undertakings, some through resignation
MONITORING • Approximately 1500 MDs are being monitored by College as part of registration, remediation, health or discipline processes • Of these, with respect to health: • PHP – 119 (substance misuse &/or psychiatric) • Non- PHP - 71 • Psych - 36 • General Health – 35 • Some will have preceptors/supervisors in addition to health monitors • Reports from health monitors, preceptors, supervisors, assessors, and the Physician Health Program and reports about compliance with educational/remediation plans
PHYSICIAN HEALTH PROGRAM • OMA – PHP – 1995 • CPSO – Memorandum of Understanding – 1998 • Started with substance use issues • Psychiatric issues • College has representation on Program Advisory Panel and Clinical Advisory Panel • Financial contribution • Audit planned to review whether objectives are being met and public is protected
PHYSICIAN HEALTH PROGRAM • PHP contract – addictions monitoring (abstinence model) or psychiatric monitoring or concurrent • They manage but do not treat • Arrange for assessments, monitors and drug testing • Report to College if breach of contract or risk of harm • Undertaking with College to attend PHP and follow their recommendations • If uncertain, advisory panel makes recommendations • College has representation on this advisory panel
STATUS OF REGISTRATION (AFTER INTERVENTION) Restricted* Suspended Unaffected Unaffected *Restricted privileges to prescribe narcotics
PHP CPSO Healthy Doctors Patient Safety • Physician Focus • Doctors’ Health • Confidentiality • Legislative Mandate • Public interest Responsibility
CPSO RELATIONSHIP TO PHP • “Arm’s length” • Reporting obligations clearly defined • Balance confidentiality against public safety • Memorandum of Understanding • Based upon mutual understanding, confidence and trust
BLOOD BORNE PATHOGENS • Members required to disclose if they are doing Exposure Prone Procedures (EPPs) • If doing EPPs, members are required to be tested annually for HCV, HBV, or HIV • If positive, members required to inform the College
CDC DEFINITION • BBP: Hepatitis B virus, Hepatitis C virus and HIV • Exposure-prone procedures : • Invasive procedures where there is “digital palpation of a needle tip in a body cavity…or the simultaneous presence of the HCW’s fingers, a needle or other sharp instrument or object in a blind or highly confined anatomic site… • Repair of major traumatic injuries • Manipulation, cutting or removal of any oral or perioral tissue including tooth structures….” - CDC 1998
SHEA GUIDELINES – EXAMPLEShttp://www.shea-online.org/Assets/files/guidelines/BBPathogen_GL.p • Category 1 – De minimisrisk • Gloved oral exam • Routine rectal/pelvic • Minor suturing • Colonoscopy • Category 2 – Theoretic risk • Minor oral surgery • Amputations • Laparoscopic surgery • Plastic surgery • Category 3 – Definite risk (EPP) • General surgery (abdominal) • Cardiothoracic surgery • Risk of being bitten • Obstetric surgery
SHEA GUIDELINES • If MD’s viral load is below certain level, no restriction in doing EPPs • If medication is being taken to keep viral load below certain level, College will monitor and receive reports from treating MDs • MDs can do EPP • If MD’s viral load > recommended level, MDs are restricted from EPP
BLOOD BORNE PATHOGENS • Other professional organizations acknowledge MD has ethical obligation to know his/her status • We inquire if EPP-performing MD has been tested to confirm that MD has met his/her obligation • If MD tests positive, we require monitoring to ensure that viral levels are below a set level
THE EXPERT PANEL • If doing EPPs and MD is positive, then matter is reviewed by expert panel • Comprised of experts in surgery, public health, infectious disease, a chief of staff, and others including own specialty as required • Physician has opportunity to make representations and present his or her own expert’s opinion
IF RESTRICTIONS • Restrictions only imposed if other options will not be sufficient to protect public • Restrictions will need to be shared with hospital • Restrictions may be needed while a plan is being developed
BLOOD BORNE PATHOGENS POLICY Key Expectations
ANNUAL TESTING FOR BBPS - NEW Rationale • Mandatory requirement for testing was necessary → Ethical obligation to know one’s serological status has not resulted in regular physician testing • Lack of consensus in evidence, but patient safety, public trust and physician health required CPSO to be proactive and take position
IS THERE PRACTICE AFTER A POSITIVE TEST? YES • Practice restrictions are imposed only when other means will not ensure patient safety • Even where restrictions have been required, BBP+ physicians have remained in practice
PRACTICE ASSESSMENTS • Quality Assurance • Peer Assessment • Ontario does Peer Assessment every 10 years for all MDs, and at age 70 and thereafter every 5 years • Investigations: • Complaints if serious and/or there is concerning pattern • Registrar’s Investigations
PEER ASSESSMENT AT AGE 70, WHY? • Clear evidence that at least some cognitive abilities decline with age • High risk group • If we wait for a peer assessment every 10 years there can be significant declines in the interim
WHY 70 AND OLDER? • Older physicians may have a lower case load • less opportunity for peer review (LoboPrabhu et al) • Younger physicians may feel uncomfortable voicing concerns about older colleagues out of respect, or because the older physician may have been their mentor (LoboPrabhu et al) • Detecting subtle cognitive impairment is difficult • above-average premorbid function (cognitive reserve) (Katzman et al)
WHAT DOES THE FUTURE HOLD? How will we all as stakeholders manage the demographic bulge as it advances? How do we stakeholders ensure physician competence and public safety while treating our members respectfully and with dignity?
REPORTING OBLIGATIONS • Mandatory: • Hospitals, facilities, other • Ethical: • Treating MDs • Colleagues • Future: • Regulation to make treaters obliged to report? • Standard of care for treaters to report?