Download
1 / 69
700 likes | 803 Vues
Learn about TB diagnosis, symptoms, signs, and manifestations in children, as well as the impact of HIV co-infection. Discover key features suggestive of TB and HIV-related conditions. Understand the role of Tuberculin Skin Testing (TST) in detecting TB exposure.

E N D
MANAGEMENT OF TB-HIV CO-INFECTION BY THE RESPIRATORY/INFECTIOUS DISEASE UNIT,UCTH, CALABAR
TUBERCULOSIS IN CHILDREN • It is commonly asked why young children with tb are not infectious. • They generally have a closed infection • They do not have significant cough. • They lack tussive force necessary to suspend infectious particles in the air. • When cough is present children rarely produce sputum • When sputum is produced, organisms are sparse because they are in low concentration in the endobronchial secretions of children.
Diagnosis of TB in children- The Traditional Diagnostic prerequisites • Combination of : • Contact with infectious adult case • Symptoms and signs • Positive tuberculin skin test (TST) • Suspicious CXR • Bacteriological confirmation • Serology
List of symptoms that may suggest TB in children: • Fever (Low or high grade), not responding to anti-malaria treatment • Weight loss, Static weight or failure to gain weight • Failure to thrive • Recent febrile illness with rash & desquamation (measles, persistent/continuous cough with vomiting (pertussis)
List of Suggestive Symptoms,continued • Loss of appetite • Lymph node swellings • Angle deformity of the spine (back swelling) • Joint or bone swellings • Neck stiffness, vomiting, convulsions, impaired conscious (TB meningitis)
List of possible Physical signs • Chronically or s’tmes acutely ill looking +/- pallor • Small weight for the age (underweight), or features of PEM • Discrete, or matted, frequently non-tender cervical lymphadenopathy • Features of co-existing HIV or immunocompromised status • Hypersensitivity parameters, egPhlycternularconjuctivitis, Erythema Nodosum • Manifestations of Primary Pulmonary Disease (primary complex, bronchial) • Chest signs, or features of Extra-pulmonary TB.
TB Diagnosis in children & “value” of score charts • In some countries, score charts are used for the diagnosis of TB in children but have rarely been evaluated or validated against a “gold standard” Marais BJ. Arch Dis child 2005;90:1166-70 • Score charts also perform poorly in PTB and HIV infected children! Key features suggestive of TB • The presence of 3 or more of the following should strongly suggest a diagnosis of TB: - Chronic symptoms suggestive of TB - Physical signs highly suggestive of TB - Positive TST - CXR suggestive of TB
Manifestations of TB in children • >70% of children who develop TB disease have pulmonary manifestations, but ~25 – 35% may have an extrapulmonary presentation • The most common extrapulmonary form is lymph node TB accounting for about 2/3 of cases of extrapulmonary TB • 2nd most common form is meningeal disease occurring in 13% of patients
TB-HIV COINFECTION • Manifestations of co-existent HIV-infection: • Persistent generalized lymphadenopathy, respiratory illnesses like pharyngotonsilitis, otitis media, mastoiditis, pneumonias, painless parotid enlargement. • Gastrointestinal conditions like oropharyngeal candidiasis, diarrhoea, vomiting
Other HIV-related Conditions • Pneumocystis pneumonia • Oesophagealcandidiasis • Extrapulmonarycryptococcosis • Invasive salmonella infection • Lymphoid interstitial pneumonitis • Herpes Zoster (shingles) • Kaposi’s Sarcoma • Lymphoma
Other pointers of HIV infection: • Oral: Herpes simplex, oral thrush, oral hairy leucoplakia • Cutaneous: Chickenpox, molluscum contangiosum - Delayed developmental milestones • Severe progressive encephalopathy
History - Evaluation • Careful history (including carefully extracting a history of TB contact) • Symptoms: commonest: - Chronic cough > 21 days - Fever T > 38oC for 14 days after excluding common causes, such as malaria or pneumonia - Wt loss or FTT • Some children with TB infection may not develop any signs or symptoms at any time
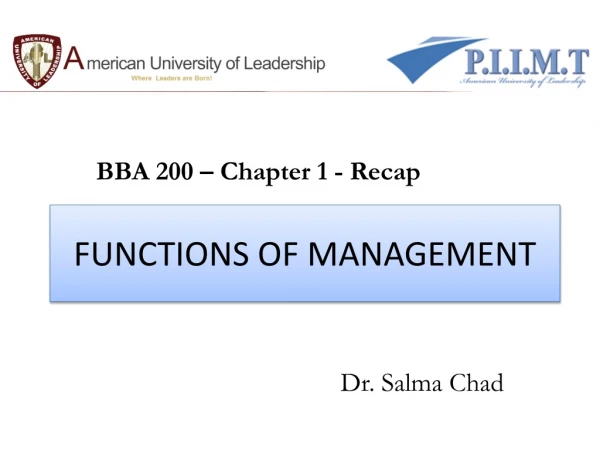
Clinical features of HIV infection and associated conditions Severe wasting Non-specific dermatitis National Paediatric ART Training Slides Unit 4 13
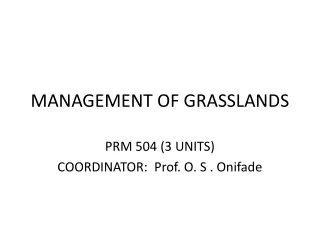
Clinical features of HIV infection and associated conditions cont…. Dermatomal Herpes zoster National Paediatric ART Training Slides Unit 4 17
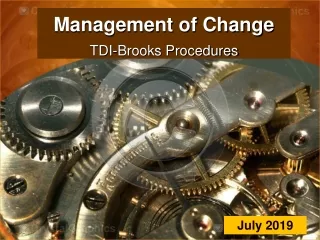
Clinical features of HIV infection and associated conditions cont…. Oral candidiasis National Paediatric ART Training Slides Unit 4 15
TST is the method used for detecting whether an individual has come in contact with the TB bacilli. The TST used is the Mantoux test, containing 5 tuberculin units administered intradermally. The test is read as mm of induration at 48 to 72 hours. Tuberculin Skin Testing (TST)
Mantoux Test • A positive test occurs when a person is infected with M. tb but does not necessarily indicate disease • Interpretation: - 0 – 4mm = negative - 5 – 9mm = borderline - ≥ 10mm = positive in all other children irrespective of the BCG vaccination - ≥ 5mm = positive in HIV infected children and severely malnourished children (marasmus, kwashiorkor) • Useful in screening household contacts with TB • Fewer HIV infected children will have a positive TST • TST may be negative initially but positive after 2-3 mo of treatment
Chest Radiograph as a diagnostic tool of TB • Spectrum of radiolographic changes depends on the stage of the disease & the nature of the intrathoracic complications • There are no pathognomonic radiological signs of tuberculosis; other lung lesions (viral, bacterial & fungal LIP & IPH) can mimic those of pulmonary TB. • Additional radiographs like cervical, spinal/vertebral & abdominal may also be required
Chest Radiograph as a diagnostic tool of TB - 2 • Certain radiological lesions may however suggest PTB: - Miliary mottling - Hilar or paratracheallymphadenopathy - ± parenchymal involvement - Collapse consolidation - Pleural effusion • Cavitatory lesions are rare, but should nevertheless be looked for, • Rarely chest X-ray may be normal
Radiological Picture of LIP • Diffuse bilateral reticulonodular infiltrates may appear similar to miliary TB • Bilateral hilar or mediastinal lymph node enlargement
LIP Miliary TB LIP vs Miliary TB
Isolation of TB bacilli from clinical specimens remains the gold standard for diagnosis Isolation in children is more difficult than in adults, as they have paucibacillary disease The yield of the organism is low even in the best centres (<50%). Bacteriological diagnosis in children
Specimen collection 1.Sputum : - 10 years or older who can expectorate an on the spot specimen, an early morning specimen and another on the spot specimen 2. Gastric aspiration (fasting, early morning) - Aspiration of gastric contents should be performed fasting, ideally while still recumbent after overnight sleep. - Therefore usually performed in hospitalized patients. - Strict adherence to the recommended collection techniques improves the yield of the procedure, as does the collection of specimens on three consecutive days.
Specimen collection-1 3. Induced sputum • The use of nebulized hypertonic saline to induce coughing allows the production of respiratory specimens in children who cannot expectorate voluntarily • Yield from 1 induced sputum specimen = 3 daily gastric aspirates, and is ↑ further by repeated procedures • 149 children hospitalized pneumonia, Zar 2000 • median age 9 (3-30) months • IS in 142 (95%) • Induced Sputum positive in 15(10.6%) vs 9 Gastric Lavage (6.3%), p=0.08
Specimen collection -2 • Broncho-alveolar lavage • Fine needle aspiration (FNA): of enlarged glands for AFB and cytology – has a high bacteriological yield 6. Biopsy
Other diagnostic parameters • FBC and ESR- may be normal but commonly leucocytosis with a relative lymphocytosis and a high ESR • BCG test • Normal BCG evolution • Accelerated BCG reaction
Novel/Recent Advances in TB Diagnosis
Lipoarabinomannan (LAM) assay • Antigen capture ELISA assays for the detection of lipoarabinomannan (LAM) in sputum and urine samples has shown promise in suspected TB adults (Boehme C et al, Trans Roy Soc Trop Med Hyg 2005;99:893-900) • LAM is a cell wall lipopolysaccharide antigen specific for M. tuberculosis • Released from metabolically active or degrading cells • Secreted intact in urine • Results are rapid, typically within 2-3 hours • 76.5% sensitive in smear negative cases, 80.3% sensitive overall, 99% specific • Performs well in the HIV-infected subgroup
Interferon Gamma Release assays (IGRA) • New in-vitro test which measures interferon production by T-cells • Principle: sensitised T cells produce interferon when mycobacterial Ags are encountered • M. tuberculosis-specific Ags • Available IGRA-based Tests: 1. Quantiferon-TB - IFN production (pg/ml) 2. T SPOT-TB - Detects number T cells producing IFN
TST vs IFN assays: traditional vs novel TST IFN Sensitivity 75-90%* 80-95%* Specificity 75-90% 95-100% Cross react BCG Yes No Cross react NTM Yes No Boosting Yes No Cost Low Moderate Patient visits 2 1 Lab no yes * Less in the immunocompromised (Nahid, Proc Am Thorac Soc, 2006)
Concerns with IFN assays • Cannot distinguish latent from active disease • Few studies in children • ? efficacy in very young/ HIV/ high incidence TB countries • Discordance with TST results – Pai Lancet Infect Dis 2004, Mahomed IJTLD 2006 • ? impact of TB treatment • Need for laboratory • Cost • Promising and more sensitive than TST
Other Newer M. tuberculosis detection methods • BACTEC offer slightly superior sensitivity and reduced turn around times compared with conventional Loweinstein –Jensen medium (LJ-medium) • MODS( microscopic observation drug susceptibility assay) 8 days to culture positivity • limited utility in children • PCR: limited utility in children and low sensitivity in paucibacillary TB • NAAT (nucleic acid amplification test) rapid test (WHO endorsed): 100mins • TB fluorescence microscopy • Gene expert tb test
TB/HIV co-infection in children • Should HIV testing be done in all children suspected of having TB (Yes) • Should all HIV+ve children be screened for TB? (Yes) • How do you differentiate HIV associated lung disease from TB disease? • Can children with HIV lung disease also have TB disease? (Yes)