Download
1 / 15
150 likes | 242 Vues
Explore the practical implementation of ESPGHAN/ESPEN Guidelines 2005 in neonatal parenteral nutrition, citing expert opinions and best practices for optimizing patient care. Understand challenges and recommendations for standardized solutions in clinical scenarios.

E N D
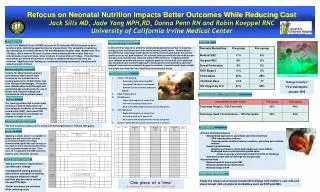
Neonatal Parenteral Nutrition – putting the guidelines into practice Sarah Dunnett Senior Pharmacist & Medical Affairs Manager, Baxter UK/NUMETA/12-0024 Peter Mulholland Neonatal Pharmacist, Southern General Hospital NPPG Roundtable – November 2012
ESPGHAN/ESPEN Guidelines 2005 • Cited by Chief Pharmacists Report • Consensus of credible professional bodies & authoritative individuals • International WP of HCPs actively treating patients - dietitians, pharmacists, nurses, paediatricians (gastroenterology), neonatology, biochemists, microbiologists • Acknowledge PN as one of the most important therapeutic advances in paediatrics over the last 3 decades ‘Guidelines do not provide answers to every clinical question; nor does adherence to guidelines ensure a successful outcome in every case’ (S2) Journal of Paediatric Gastroenterology and Nutrition 41:S1-S87 November 2005
ESPGHAN/ESPEN Guidelines 2005 • Acknowledge scarcity of good quality clinical trials in children • Apply paed studies + adult studies + expert opinion • Apply Scottish Intercollegiate Guideline Network ratings of evidence base Grading of Recommendation • GORA: Strongest evidence base eg high quality meta -analyses, systematic reviews of randomised controlled trials eg minimum 1.5g/kg/day amino acid to prevent negative nitrogen balance in pre-terms (S14) • GORB: A consistent body of evidence eg systematic review of case-control or cohort studies eg IV lipid no later than day 3 but may be started on the first day of life (S23), continuous 24hour lipid infusion for infants, newborns and premature babies (S20) • GORC: A body of evidence eg case-control or cohort studies eg max glucose of 18g/kg/day for term-2years (S29) • GORD: Case reports, case series, expert opinion eg regularly check peripheral infusions for signs of extravasation (S68) • Some parameters remain undefined eg no recommendation for magnesium requirement for premature neonates (S44)
Paediatric Chief Pharmacist Report 2011 • Commissioned by DoH / 4 CPhO • Expert project team + 3 surveys → 59 best practice recommendations • 42 are the responsibility of Hospital Chief Executive or Chief Pharmacist. • Technical / Operational or Clinical • 35 are ‘must’ • 7 are ‘should’ • 17 are asks of external bodies • Taking stock 1 year post publication…
Paediatric Chief Pharmacist Report 2011 • Recommendations across the full pathway of care eg • Accountability for treatment decisions • Capacity and competency assessments • Evidence based, ratified local guidelines with annual review • Monitoring protocol and accountabilities • Standardised electronic documentation • Aseptic service role and standards • Issue tracking and management • Consistent with NCEPOD report • Unnecessary variation in neonatal PN practice between units, particularly for ELBW neonates. ‘Greater use of standardised PN solutions has an important role to play in facilitating change in practice and maintaining capacity to provide PN within the NHS’
Collaboration with external partners Paediatric Chief Pharmacist Report 2011 egNumeta
Clinical scenario - responding to results 700g / 27 week gestation Assume other results ‘normal’ What is your most probable course of action? Add Na via burette ↓ PN infusion rate to ↓ fluid volume ↑ Na in next PN ↑ Na in next PN and transition to new bag earlier than usual No change Other… Neonatal plasma Na ref range 133-146mmol/l
Clinical scenario - responding to results 700g / 27 week gestation Assume other results ‘normal’ What is your most probable course of action? Add Na via burette ↓ PN infusion rate to ↓ fluid volume ↑ Na in next PN ↑ Na in next PN and transition to new bag earlier than usual No change Other… Neonatal plasma Na ref range 133-146mmol/l Demonstrates multi-factorial challenges… Highlights value of developing algorithms to facilitate optimum, consistent clinical decisions
Neonatal Pharmacy – NPPG Survey 2012 Clinical Service Provisionn = 72 Aseptic Service Provisionn = 70 • Points to ponder: • Appears that Clinical Service is offered on less days than Aseptic Service – Why? • Consider sustainability and capacity planning locally - Is my Clinical and Aseptic Service provision aligned? If not, do we have a gap? • What can we learn from centres providing 7days per week Aseptic or Clinical Services?
Neonatal Additions – NPPG Survey 2012 • Are additions ever made at ward level to the PN after preparation? Yes = 14/75 • If Yes, how is this done? (NB: Some multiple responses) • Burette = 7/18 • Into PN bag = 1/18 • Separate infusion/bolus = 10/18 • Points to ponder: • Do you have a protocol defining the method for each type of addition? • How are calculations and stability verified? • How do you manage the giving set priming volume?
Self-audit to the recommendations Document who is responsible/ accountable / to be consulted / to be informed
Self-audit to the recommendations Document who is responsible/ accountable / to be consulted / to be informed
Numeta Range Prescribing Information Name & Composition: Numeta G13%E & G16%E emulsion for infusion. Reconstituted triple chamber bag contains:Numeta G13%E Active Substance:Amino Acid Chamber :Alanine 0.75g, Arginine 0.78g, Aspartic acid 0.56g, Cysteine 0.18g, Glutamic acid 0.93g, Glycine 0.37g, Histidine 0.35g, Isoleucine 0.62g, Leucine 0.93g, Lysine monohydrate (equivalent to Lysine) 1.15g (1.03g), Methionine 0.22g, Ornithine hydrochloride (equivalent to Ornithine) 0.30g (0.23g), Phenylalanine 0.39g, Proline 0.28g, Serine 0.37g, Taurine 0.06g, Threonine 0.35g, Tryptophan 0.19g, Tyrosine 0.07g, Valine 0.71g, Potassium acetate 0.61g, Calcium chloride dehydrate 0.55g, Magnesium acetate tetrahydrate 0.27g, Sodium glycerophosphate hydrated 0.98g. Glucose Chamber: Glucose monohydrate (equivalent to glucose anhydrous) 44.00g (40.00g). Lipid Chamber: Refined olive oil (approximately 80%) + Refined soya bean oil (approximately 20%) 7.5g.Numeta G16%E Active Substance:Amino Acid Chamber :Alanine 1.03g, Arginine 1.08g, Aspartic acid 0.77g, Cysteine 0.24g, Glutamic acid 1.29g, Glycine 0.51g, Histidine 0.49g, Isoleucine 0.86g, Leucine 1.29g, Lysine monohydrate (equivalent to Lysine) 1.59g (1.42g), Methionine 0.31g, Ornithine hydrochloride (equivalent to Ornithine) 0.41g (0.32g), Phenylalanine 0.54g, Proline 0.39g, Serine 0.51g, Taurine 0.08g, Threonine 0.48g, Tryptophan 0.26g, Tyrosine 0.10g, Valine 0.98g, Sodium chloride 0.30g, Potassium acetate 1.12g, Calcium chloride dehydrate 0.46g, Magnesium acetate tetrahydrate 0.33g, Sodium glycerophosphate hydrated 0.98g. Glucose Chamber: Glucose monohydrate (equivalent to glucose anhydrous) 85.25g (77.50g). Lipid Chamber: Refined olive oil (approximately 80%) + Refined soya bean oil (approximately 20%) 15.5g. If lipids not required, bag design allows activation of peel seals between amino acids/electrolytes and glucose chambers only. Indications: Parenteral Nutrition when oral or enteral nutrition is not possible, insufficient or contraindicated: Numeta: G13%E - preterm newborn infants, G16%E - term newborn infants and children up to 2years. Dosage and Route: Dependant on clinical condition and metabolism. Continue for as long as clinically required. Administer via central vein; or dilute with sufficient water for injection for peripheral infusion. Adjust administration rate gradually, according to formulation used, dosage, daily volume intake and duration of infusion. Side effects:see Summary of Product Characteristics (SPC) for detail.Hypophosphataemia, Hyperglycaemia, Hypercalcaemia, Hypertriglyceridaemia, and Hyponatraemia. Fat overload syndrome (reversible when lipid infusion stopped). Precautions: Stop infusion immediately if signs or symptoms of allergic reaction develop (fever, sweating, shivering, headache, skin rashes or dyspnoea). Refeeding syndrome (characterised by shift in intracellular electrolytes), thiamine deficiency and fluid retention may also develop. Correct fluid, electrolyte and metabolic disorders before use. Lipids, vitamins, electrolytes and trace elements should be administered as required. Follow aseptic procedures for additions. Check compatibility of additions – risk of occlusion from precipitate formation. With additions the final osmolarity must be measured before administration via peripheral vein to avoid vein irritation. Routinely monitor water and electrolyte balance, serum osmolarity, triglycerides, acid/base balance, blood glucose, hepatic and renal function, blood count and coagulation parameters throughout treatment. Adjust administration to meet clinical needs in unstable conditions (e.g. following severe post-traumatic conditions). Caution in pulmonary oedema, heart failure, hepatic insufficiency, renal insufficiency and severe blood coagulation disorders. Monitor for endocrine and metabolic complications. Fat overload syndrome may develop. Contraindications: As activated 2 chamber bag - hypersensitivity to egg, soy or peanut proteins, or any active substances, excipients, or components of the container; congenital abnormality of amino acid metabolism; significantly raised electrolytes; severe hyperglycaemia. As above for the activated 3 chamber bag (with lipids) also, severe hyperlipidaemia or severe disorders of lipid metabolism characterized by hypertriglyceridemia. Interactions: Do not administer simultaneously with blood through same infusion tubing due to risk of pseudoagglutination. Do not co-administer with ceftriaxone, take special care with coumarins & their derivatives, potassium sparing diruretics and ACE Inhibitors. Lipids may interfere with certain laboratory tests if the sample is taken before they have cleared. Overdose: In the event of incorrect administration, overdose and/or excessively fast rate, signs of hypervolaemia and acidosis, hyperglycaemia, glycosuria and a hyperosmolar syndrome may occur. Nausea, vomiting, shivering and electrolyte disturbances may develop. Fat overload syndrome may result. Stop infusion immediately. Emergency procedures should be general supportive measures, particular attention to respiratory and cardiovascular systems. Legal Category: POM Marketing Authorisation Holder: Baxter Healthcare Limited, Caxton Way, Thetford, Norfolk IP24 3SE Numeta G13%E: Marketing Authorization: PL 00116/0647. Code: FDB9601. Basic NHS Price: £73.04. Numeta G16%E: Marketing Authorization: PL 00116/0648. Code: FDB9612. Basic NHS Price: £84.35 Date of preparation: September 2012Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Any adverse events relating to Baxter products can also be reported direct to Baxter Pharmacovigilance on 01635 206360, or by email to vigilanceuk@baxter.com
Neonatal Parenteral Nutrition – putting the guidelines into practice Review status and actions against the Paediatric Chief Pharmacist Report + associated recommendations Recognise value of clear documentation locally Opportunity for collaboration and sharing best practice NPPG Roundtable – November 2012