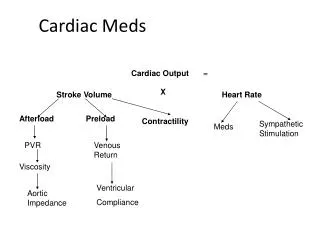
Management of Cardiovascular Intoxication Cases with Beta-Blockers and Calcium Channel Blockers
500 likes | 540 Vues
Learn about the principles of disease pathophysiology, manifestations, complications, diagnostic strategies, and management of beta-blocker and calcium channel blocker intoxication. Includes case studies and treatment options.

Management of Cardiovascular Intoxication Cases with Beta-Blockers and Calcium Channel Blockers
E N D
Presentation Transcript
Cardiovascular Meds Intoxication Zohair Al Aseri MD,FRCPC EM & CCM
Beta Blockers & Ca Channels Blockers Intoxication Cardiovascular Tox Zohair Al Aseri MD,FRCPC EM & CCM
Introduction Case 1 • a 64-year-old man who took an overdose of his medications. Zohair Al Aseri MD,FRCPC EM & CCM
Case 1 • has a history of hypertension, atrial fibrillation, and depression. • lethargic but arousable • reports he took about 40 tablets of immediate-release metoprolol three hours ago in an attempt to “end it all.” Zohair Al Aseri MD,FRCPC EM & CCM
Case 1 • “Is this a lethal overdose? • If he is symptomatic, which therapy will you try first, and what are your options?” Zohair Al Aseri MD,FRCPC EM & CCM
Case 2 • a 2-year-old child in the pediatric area who was found playing with grandma’s bottle of verapamil controlled release 15 minutes ago. • The grandmother thinks that at most there are three tablets missing. Zohair Al Aseri MD,FRCPC EM & CCM
Case 2 Child looks great • “Are three tablets a big deal? • Can we just watch the child for a couple of hours? • Do we need an IV and blood work? Zohair Al Aseri MD,FRCPC EM & CCM
Principles of Disease Pathophysiology B. Blockers • Inhibit endogenous catecholamines such as epinephrine at the beta-receptor. Zohair Al Aseri MD,FRCPC EM & CCM
Selected Characteristics of Common Beta-Blockers Zohair Al Aseri MD,FRCPC EM & CCM
Principles of Disease Pathophysiology B. Blockers • Rapidly absorbed after oral ingestion • Peak effect of normal-release preparations occurs in 1 to 4 hours. Zohair Al Aseri MD,FRCPC EM & CCM
Principles of Disease Pathophysiology B. Blockers • Hepatic metabolism on first pass results in significantly less bioavailability after oral dosing than with IV injection (1 : 40 for propranolol). • Volume of distribution for various beta-blockers generally exceeds 1 L/kg, meaning tissue concentrations exceed those of serum. hemodialysis is not efficacious for most beta-blockers Zohair Al Aseri MD,FRCPC EM & CCM
Principles of Disease Pathophysiology Principles of Disease Pathophysiology B. Blockers • Protein binding varies from 0% for sotalol to 93% for propranolol. • Elimination half-lives vary from 8 to 9 minutes for esmolol to as long as 24 hours for nadolol and others Zohair Al Aseri MD,FRCPC EM & CCM
MANIFESTATIONS AND COMPLICATIONS OF BETA-BLOCKER OVERDOSEIN ORDER OF DECREASING FREQUENCY Zohair Al Aseri MD,FRCPC EM & CCM
Diagnostic Strategies • Depend on the clinical picture • Hypoglycemia is common in children Zohair Al Aseri MD,FRCPC EM & CCM
Management B. Blockers Intoxication • IV fluids • Oxygen • Monitoring of cardiac rhythm and respirations. • Activated charcoal is unproven treatment. • Multiple-dose charcoal without supporting evidence for an improvement in outcome. Zohair Al Aseri MD,FRCPC EM & CCM
Management Management B. Blockers Intoxication • Absence of symptoms 4 hours after ingestion implies a low risk for subsequent morbidity unless a delayed-release preparation is involved. Zohair Al Aseri MD,FRCPC EM & CCM
Management Management B. Blockers Intoxication Hypotension, Bradycardia, and Atrioventricular Block • Fluid & Catecholamines Zohair Al Aseri MD,FRCPC EM & CCM
Management Management B. Blockers Intoxication The first step in the treatment of beta-blocker overdose is • Atropine • Glucagon • Crystalloid fluids. Zohair Al Aseri MD,FRCPC EM & CCM
Management Management B. Blockers Intoxication • In hypotensive patients, 20 to 40 mL/kg of normal saline or Ringer's lactate solution can be infused and repeated. • If hypotension or bradycardia persists, other cardioactive drugs are indicated. • dopamine, or epinephrine. Zohair Al Aseri MD,FRCPC EM & CCM
Management Management B. Blockers Intoxication • Other catecholamines include norepinephrine, dobutamine, and phenylephrine. • Often, norepinephrine or dopamine is added to beta-agonists such as isoproterenol that lack vasopressor activity. Zohair Al Aseri MD,FRCPC EM & CCM
TREATMENT OF BETA-BLOCKER POISONING Zohair Al Aseri MD,FRCPC EM & CCM
Management B. Blockers Intoxication Disposition • Patients who remain completely asymptomatic for 6 hours after an oral overdose of normal-release preparations can be safely referred for psychiatric evaluation, with medical consultation for the first 24 hours. Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Perspective • Most fatalities occur with verapamil Zohair Al Aseri MD,FRCPC EM & CCM
Pathophysiology CALCIUM CHANNEL BLOCKERS Calcium channel antagonists • block the slow calcium channels in the myocardium and vascular smooth muscle, leading to coronary and peripheral vasodilation. • reduce cardiac contractility • depress SA nodal activity • slow AV conduction. Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Pathophysiology • Both verapamil and diltiazem act on the heart and blood vessels, whereas nifedipine causes primarily vasodilation. • In the pancreas, calcium channel blockade inhibits insulin release, resulting in hyperglycemia. • As with beta-blockers, selectivity is lost in cases of overdose Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Pathophysiology • All calcium channel blockers are rapidly absorbed • Onset of action and toxicity ranges from less than 30 minutes to 60 minutes • Peak effect of nifedipine can occur as early as 20 minutes after ingestion, Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Pathophysiology • High protein binding and Vd greater than 1 to 2 L/kg make hemodialysis or hemoperfusion ineffective. • Fortunately (except with sustained-release preparations), their half-lives are relatively short, limiting toxicity to 24 to 36 hours. Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Selected Characteristics of Some Calcium Channel Blockers Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS MANIFESTATIONS AND COMPLICATIONS OF CALCIUM CHANNEL BLOCKER POISONING Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Diagnostic Strategies • Serum levels of calcium antagonists are not available • Glucose and Electrolytes (including calcium and magnesium). • Hyperglycemia secondary to insulin inhibition occurs occasionally, but mild and short-lived requires no treatment. • Lactic acidosis occurs with hypotension and hypoperfusion. Zohair Al Aseri MD,FRCPC EM & CCM
Diagnostic Strategies • ECG • A prolonged QRS or QT interval suggests bepridil or a co-ingested cardiac toxin such as a TCA. Zohair Al Aseri MD,FRCPC EM & CCM
CALCIUM CHANNEL BLOCKERS Management • IV • O2 • Cardiac monitoring • No evidence for activated charcoal Zohair Al Aseri MD,FRCPC EM & CCM
TREATMENT OF CALCIUM CHANNEL BLOCKER INTOXICATION Zohair Al Aseri MD,FRCPC EM & CCM
Disposition • Because the peak effect occurs in 90 minutes to 6 hours, patients who are totally asymptomatic for 6 hours can be safely discharged • For delayed-release preparations should be admitted for at least 24 hours of continuous cardiac monitoring. Zohair Al Aseri MD,FRCPC EM & CCM
NITRATES AND NITRITES • Widely used as vasodilators in the treatment of heart failure and ischemic heart disease. • augment coronary blood flow as well as reduce myocardial oxygen consumption by reducing afterload. • At lower doses nitrates primarily dilate veins • At higher doses they also dilate arteries. Zohair Al Aseri MD,FRCPC EM & CCM
NITRATES AND NITRITES • Hypotension is a common complication, but usually responds to supine positioning, IV fluids, and reduction of dose. • Hypotension is usually transient. • Low-dose pressors are occasionally needed, but it is best to avoid them in the setting of acute coronary syndromes. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Intoxication Zohair Al Aseri MD,FRCPC EM & CCM
The foxglove plant, from which digitalis is derived. DIGITALIS Perspective Zohair Al Aseri MD,FRCPC EM & CCM
Principles of Disease Pathophysiology In therapeutic doses, digitalis has two effects: (1) increasing the force of myocardial contraction to increase cardiac output in patients with heart failure. (2) decreasing atrioventricular (AV) conduction to slow the ventricular rate in atrial fibrillation. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Principles of Disease Pathophysiology • It inhibits membrane sodium-potassium adenosine triphosphatase (ATPase), which increases intracellular sodium and calcium and increases extracellular potassium. At therapeutic doses, the effects on serum electrolyte levels are minimal. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Principles of Disease Pathophysiology • With toxic levels, digitalis paralyzes the Na-K pump, potassium cannot be transported into cells, and serum potassium can rise as high as 13.5 mEq/L. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Principles of Disease Pathophysiology • At therapeutic levels, digitalis indirectly increases vagal activity and decreases sympathetic activity. • At toxic levels, digitalis can directly halt the generation of impulses in the SA node, depress conduction through the AV node, and increase the sensitivity of the SA and AV nodes to catecholamines. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Principles of Disease Pathophysiology • Digitalis can produce virtually any dysrhythmia or conduction block, and bradycardias are as common as tachycardias. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis DYSRHYTHMIAS ASSOCIATED WITH DIGITALIS TOXICITY Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Principles of Disease Pathophysiology • Because significant protein binding and large volume of distribution suggest that hemodialysis, hemoperfusion, and exchange transfusion are ineffective. Zohair Al Aseri MD,FRCPC EM & CCM
Digitalis Disposition and Summary • All patients who are symptomatic for digitalis intoxication with hyperkalemia, dysrhythmia, AV block, or significant comorbidity should be admitted to the hospital or the emergency department observation unit for at least 12 hours of continuous cardiac monitoring. • All patients treated with antibodies require admission to an intensive care unit. Zohair Al Aseri MD,FRCPC EM & CCM
ED Evaluation Important to know: • time of ingestion • specific name of the medication • number of pills ingested • formulation (i.e., immediate release vs. sustained release) • dose per tablet • co-ingestants • chronic medications taken as prescribed • alcohol, or illicit drugs. Zohair Al Aseri MD,FRCPC EM & CCM