Download

1 / 62
680 likes | 1.64k Vues
Opportunistic Fung i & Pneumocystis. Doç.Dr.Hrisi BAHAR. Opportunistic organisms. Opportunistic organisms are normal resident flora that become pathogenic only when the host's immune defense reduses. I n immunosuppressive therapy, I n a chronic disease such as diabetes mellitus,

E N D
Opportunistic Fungi&Pneumocystis Doç.Dr.Hrisi BAHAR
Opportunisticorganisms • Opportunistic organisms are normal resident flora that become pathogenic only when the host's immune defense reduses. • In immunosuppressive therapy, • In a chronic disease such as diabetes mellitus, • During steroid or antibacterial therapy that upsets the balance of bacterial flora in the body.
Opportunistic Mycosis • Opportunistic mycosisis a fungal or fungus-like disease occurring in an animal or human’s with a compromised immune system. • Opportunistic fungal infections are: • CandidiasisAspergillosisCryptococcosis
CANDIDA SP • Candidia can infect skin, mucosa, or internal organs • It is as Yeast Like fungus • It is an important cause of opportunistic fungal infection.
Candida ► Candida is found in normal flora,exist in mouth, gastrointestinal tract,vagina, skin in 20 % of normal individuals. ►Colonization increases with age,inpregnancy, hospitalization….. ►Candida is an important etiological agent presenting as opportunistic infection in Diabetes and HIV patients.
Morphology and Culturing • The shape is ovoid or spherical budding cells and produces pseudo mycelium • Routine cultures are done on Sabouraud's dextrose agar, • Grow predominantly in yeast phase • A mixture of yeast cells and pseudo mycelium and true mycelium are seen in vivo and nutritionally poor media.
Candida as Pathogenic fungi Systemic Candidosis • Occurs in Patients who carry more yeasts in mouth, and gastrointestinal system, • Predisposed with individuals 1. On antibiotic or/and steroid therapy 2. Immunosupressed 3. Recipients with organ transplantation 4. Infancy – Old age – Pregnancy 5. Diabetes mellitus 7. Zink and iron deficiencies
Pathogenesis and Pathology • Mucosal infections occur superficially –Discrete white patches on mucosal surface. • Can affect tongue • Infants and old persons are affected • In Immune compromised /AIDS, oral candidois is commonly seen • Vaginal candidosis causes itching soreness white discharge, white colored lesions, • In pregnancy in advanced stage, • Majority experience one episode in a life time
Important species of Candida in human infections • C.albicans • C.tropicalis • C.glabrata • C.krusei
Many cases of AIDS are suspected by observation of oral cavity
Laboratory Diagnosis • Skin scrapings, • Mucosal scrapping, • Vaginal secretions • Culturing blood and other body fluids, • Observations Microscopic observation after Gram staining. Presence of Gram + yeast cells.
Laboratory Diagnosis • Isolation of Candida from various specimens • Easier to culture onSabouraud's dextrose agar • Serology, molecular methods,PCR
CRYPTOCOCCUS NEOFORMANS • A capsulated yeast – A true yeast.. • A sporadic disease in the past. • Most common infection in AIDS patients.
Morphology • A true yeast • Round 4 – 10 microns • Surrounded by Mucopolysaccharide capsule. • Thick in vivo • Negative staining with India Ink and Nigrosin • 60% of the infected prove positive by India Ink preparation on examination of CSF • KoH preparations in Sputum and other tissues, • PAS and Mucicaramine staining helps confirmation.
Culturing • CSF-Culturing on Sabouraud's agar, and incubated at 370C for upto to 3 weeks • Cultures appear as creamy, white, yellow brown colored *Simple urease test helps in confirming the isolate.
Cryptococcus neoformansSerotypes • A true yeast • 4 serotypes - A,B,C,D • A and D - C.neofromans var neoformans • B and C - C.neoformans var gatti. • Many infections are caused by C.neofromans var neoformans. Found in wild/Domesticated birds. Pigeons carry C.neofromans, Birds do not get infected.
Pathogenesis • Enters through lungs by inhalation of “basidiospores” of C.neoformans • Enters deep into lungs, pulmonary infections can occur. • Men acquires more infections, and women less infected. • Self limiting in most cases, • Present as discrete nodules - Cryptococcoma.
Pathogenesis • Can infect normal humans • Abnormalities of T lymphocyte function aggravates, the clinical manifestations. • In AIDS 3-20% develop Cryptococcosis. • Present with chronic meningitis , meningo encephalitis • Manifest with – head ache low grade fever, • Visual abnormalities ,Coma – fatal • Treatment reduces the morbidity and cure in non immuno supressed expected.
Clinical manifestation • 1.Pulmonary Cryptococcosis • 2.Central Nervous System Cryptococcosis • 3.Cutaneous Cryptococcosis • 4.Cryptococcosis of bone • 5.Ocular Cryptococcosis • 6.Other forms (Cryptococcus neoformans is often isolated from urine of patients with disseminated infection. Occasionally, signs of pyelonephritis or prostatitis may be observed. Other rare forms of cryptococcosis include adrenal cortical lesions, endocarditis, hepatitis, sinusitis, and localized oesophageal lesions) .
Laboratory Diagnosis. • CSF Microscopic observation under India Ink preparation • Direct microscopy - Gram staining • Cultures on Sabouraud dextrose agar, • Serological tests for detection of Capsular antigen • CSF findings mimic like Tuberculosis • IN CSF - latex test for detection of Antigen • Blood cultures, • ELISA
Treatment Immune competent Fluconazole,Itraconazole Immune Deficient Amphotericin B,Flucytosine AIDS patients are not totally cured , Relapses are frequent with fatal outcome. Rapid resistance develops with Fluconazole. Avoid contact with Birds
ASPERGILLUS SP • In nature > 100 species of Aspergillus exist, Few are important as human pathogens • 1 A.fumigatus • 2 A.niger • 3 A.flavus • 4 A.terreus • 5 A.nidulans
Morphology • Cultured as Mycelial fungus • Separate hyphae with distinctive sporing structures • Spore bearing hyphae – Conidiophores terminates in a swollen cell vesicle surrounded by one or two rows of cell ( Streigmata ) from which chains of asexual conidia are produced
Pathogenesis Clinical presentations • Allergic Aspergillosis – Atopic individuals, with elevated IgE levels • 10-20% of Asthmatics react to A.fumigatus • Allergic alveoitisfollows particularly heavy and repeated exposure to larger number of spores • Maltsters Lung – causes allergic alveolitis, who handle barley on which A.claveus has sporulated during malting process
Pathogenesis • Aspergilloma– A fungal ball, fungus colonize Preexisting (Tuberculosis ) cavities in the lung and form compact ball of Mycelium which is later surrounded by dense fibrous wall presents with cough, sputum production • Haemoptysisoccurs due to invasion of blood vessels
Pathogenesis Invasive Aspergillosis occurs in immunocompromised host with underlying disease • Neutropenia is the most common predisposing factor • A.fumigatus is the most common infecting species • In bone marrow recipients leads to high mortality • Fungus invades blood vessels, causes thrombosis septic emboli • Can spread to Kidney and heart.
ZYGOMYCETES • The ilness is calledZygomycosis,also called asMucor Mycosis or Phycomycosis • Saprophytic mould fungi • Major Causative agents ofZygomycosis Rhizopus Mucor Absidia
Morphology • Majority are with broad aseptate mycelium with many number of asexual spores inside a sporangium which develops at the end of the aerial hyphae
Mucor • Microscopy ► Non septate hyphae ►Having branched sporangiophores with sporangium at terminal ends
Rhizopus Microscopy ►Shows non septate hyphae ►Sporangiophores in groups are above the Rhizoids
Important Clinical Manifestations • Rhino cerebral Zygomycosis associate with Diabetus mellitus, leukemia, or lymphomas • Causes extensive Cellulitis, and tissue destruction.
Mucormycosis • Cellulitis causes extensive tissue destruction. • Spread from nasal mucosa to turbinate bone,paranasal sinuses ,orbit, and brain • Rapdily fatal if untreated
Laboratory Diagnosis Histopathology more reliable than culturing
Pathology and Pathogenesis • Spread from nasal mucosa • Spread to turbinate bones,para nasal sinuses , orbit, brain • Associated with uncontrolled diabetes mellitus • In leukemia patients , Lymphoma patients, • Leads to fatal outcome, • Improved with anti fungal treatment. • Spread to lungs disseminated infection,.
Treatment • Early Diagnosis highly essential for effective cure • High doses of I V Amphotericin B • Surgical interventions • Control of Diabetes a basic requirement for better clinical outcome
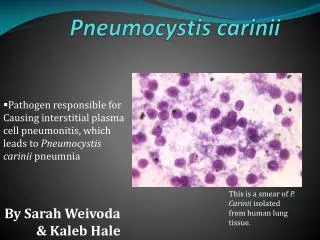
PNEUMOCYSTIS Identified as the most Important opportunistic fungal infection in persons with impaired immune systems & AIDS
Pneumocystis • Pneumocystis is a genus of unicellular fungi found in the respiratory tracts of many mammals and humans. • The organism was first described in 1909 by Chagas and then a few years later by Delanöes, who ultimately named the organism in honor of Dr. Carini after isolating it from infected rats. • The name wasPneumocystis carinii
Pneumocystis • Years later, Dr. Otto Jirovec and his group isolated the organism from humans, and the organism responsible for P.carinii pneumonia (PCP) was renamed after him andP.carinii change to Pneumocystis jiroveci
Pneumocystis • The taxonomic classification of the Pneumocystis genus was debated for some time • It was a trypanasome then a protozoan and today it is accepted as a fungus. • The organism is found in 3 distinct morphologic stages, as follows: The trophozoite (trophic form), The sporozoite (precystic form)and the cyst, which contains several intracystic bodies
Pneumocystis jiroveci pneumonitis (PCP) is a common opportunistic disease that occurs almost exclusively in persons who have profound immunodeficiency.PCP was and still is the most common life-threatening opportunistic infection occurring in patients with HIV disease. Pathogenesis
Pathogenesis ►The portal of entry for P carinii has not been firmly established; however, because the organism has been found only in the lung, inhalation is a likely mode of transmission. ►In most individuals, the organism is dormant and sparsely dispersed in the lung, with no apparent host response (latent infection). ►In susceptible (immunocompromised) hosts, the organism occurs in massive numbers.