Download
1 / 29
290 likes | 424 Vues
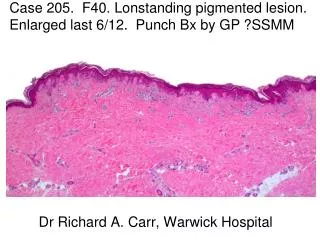
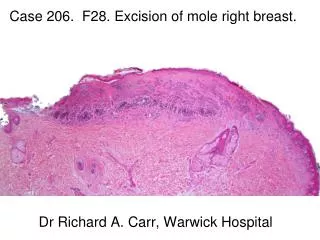
Case 206. F28. Excision of mole right breast. Dr Richard A. Carr, Warwick Hospital. Slice 1. Slice 2. Slice 3. Summary: N=53. Benign: 29 DN 21 CN 5 Clonal 1 Uncertain Favour Benign: 5* CN & Clonal 1 Unclassified 4 Uncertain Favour Malignant: 4

E N D
Case 206. F28. Excision of mole right breast. Dr Richard A. Carr, Warwick Hospital
Summary: N=53 • Benign: 29 • DN 21 • CN 5 • Clonal 1 • Uncertain Favour Benign: 5* • CN & Clonal 1 • Unclassified 4 • Uncertain Favour Malignant: 4 • Min. Dev.: 1; in situ NOS: 1; SSMM : 1; Unclassified: 1 • Malignant 18 • SSMM: 10; Min. Dev. 4; Unclassified: 3: Nodular: 1 * Includes some cases marked benign and malignant!
Parameters (N=18) • Clark level I II III IV V 4 2 7 6 0 • Breslow: 0.3 to 1.1 (Mean: 0.85; Median 0.9) • VGP: 13 RGP: 5 • Regression: Yes: 9 No: 9 • Mitoses: Absent: 13: Low: 3: High: 0 * Some parameters not assessed for melanoma in situ
EQA Participants - 1 • Sections not to full face in our circulation, so cannot be assessed in entirety. However, looks strongly sugegstive on naevoid MM arising in severely dysplastic naevus. Would do the usual workup (levs +/- Ki 67, ? p16) • I need some history! One section looks like a dysplastic junctional nevus, one looks like a sclerosed, traumatised nevus with worrying adjacent junctional areas, the other which at low power looks relatively benign, has some large atypical cells in the base ??ancient nevus features.
EQA Participants • Special site naevus but with some degree of atypia and regression. Not sure if to much atypia considering the site. • Severely dysplastic naevus. If the patient was older would be more concerned about naevoid melanoma • moderately dysplastic naevus excised with narrow margin, would recommend further excision.
EQA Participants • Underlying benign conventional naevus in dermis. Junctional atypia probably still random widespread, rather than diffuse. Architectural features supportive of DN. Not much variation in nest size to suggest special site naevus. • diificult lesion - ?traumatised; there is also regression/fibrosis, most likely benign, no deep mitoses
EQA Participants • Poor sections with parts missing. The junctional component shows shouldering, architectural and cytological atypia. Melanoma in-situ I think. The dermal compnent seems to be maturing. • Difficult - at least melanoma in-situ, incompletely excised, arising in a naevus with regression • An example I think of so called special site naevus.
EQA Participants • This is a difficult case but on balance I think this is a benign naevus of special site type (naevus of special site) which has been traumatised • Differential between dysplastic nevus and special site nevus. Dysplastic nevus favoured. • difficult case- background atypical compound naevus with evidence of regrssion and possible trauma at one edge
EQA Participants • Specimen traumatised and difficult to assess. However even though naevi in the breast area allowed more atypia, the atypia and the architecture is too atypical for this to be benign.Cells look naevoid. • Compound naevus in special site skin, so allowances to be made in terms of architecture for that. Nonetheless, I think that there is cytological atypia and would regard this as a dysplastic naevus
EQA Participants • Superficial fibrosis • ulcerated??traumatised compound melanocytic lesion showing areas of subepidermal fibrosis ??regression??previous curretage of lesion. Morte worrying lesion but on balance benignprobably dysplastcic • I find the marked assymmetry of this lesionconcerning, but having said that I don't think the cytology or architecture of either component is bad enough to call melanoma.
EQA Participants • Special site naevus, traumatised. • Elongation and fusion of rete ridges, cytological atypia. Dermal component shows regression but appears maturing with no mitosis. Some sections are incomplete so need to ask for deeper levels. • Special site naevus • Complex lesion m.i.s., regression, naevus with dermal component & mild dysplasia
Slide Club “Experts” • site related atypia x1 • Dysplastic naevus x1