Download
1 / 28
290 likes | 623 Vues
Morquio A: Musculoskeletal manifestations. Morquio A patients present with marked musculoskeletal abnormalities . Skeletal dysplasia Spinal abnormalities Pectus carinatum Hip dysplasia Genu valgum Ankle valgus Hand abnormalities Flat facial features Mandibular protrusion Short stature

E N D
Morquio A patients present with marked musculoskeletal abnormalities • Skeletal dysplasia • Spinal abnormalities • Pectus carinatum • Hip dysplasia • Genu valgum • Ankle valgus • Hand abnormalities • Flat facial features • Mandibular protrusion • Short stature • Joint instability • Joint subluxation • Joint degeneration • Abnormal gait • Weak hand grip Left image: Kalteis et al, Arthroscopy, 2005 Top and bottom right images: Atinga et al, J Bone Joint Surg Br, 2008
Musculoskeletal abnormalities are the most common presenting features in Morquio A % Subjects n = 325 subjects Data based on medical history reviews MorCAP Baseline data Harmatz et al, Mol Genet Metab, 2013
Musculoskeletal abnormalities are the most common presenting symptoms in Morquio A Common initial presenting symptoms in Morquio A n = 326 subjects Montano et al, J Inherit MetabDis, 2007 International Morquio A Registry
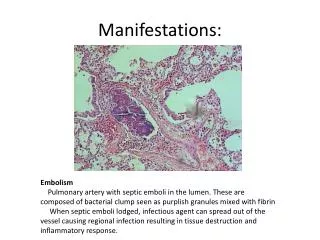
Morquio A disrupts normal development and maturation of cartilage and bone • Articular cartilage is altered in Morquio A patients: • KS accumulation in chondrocytes • Poorly organized tissue structure • Increased Type I collagen and reduced Type II collagen • Thicker, irregularly shaped collagen fibrils • Role of GAG-mediated inflammation? • Identification of biomarkers is critical for elucidation of pathogenesis Articular cartilage chondrocyte in (A) control, (B) Morquio A patient Collagen fibrils in articular cartilage of (A) control, (B) Morquio A patient Bank et al, Mol Genet Metab, 2009 Dvorak-Ewell et al, PLoS, 2010; Bank et al, Mol Genet Metab, 2009; De Franceschi et al, Osteoarthritis Cartilage, 2007; Kalteis et al, Arthroscopy, 2005; McClure et al, Pathology, 1986
Key radiographic findings in Morquio A Dysostosis multiplex (Findings vary and can be subtle)
Spine: Normal Image courtesy of Ralph Lachman, MD
Spine: Dysostosis multiplex • Dens hypoplasia • Platyspondyly • Anterior beaking • Posterior scalloping • Thoracolumbar kyphosis Solanki et al, J Inherit MetabDis, 2013
Hips: Normal Image courtesy of Ralph Lachman, MD
Hips and lower extremities: Dysostosis multiplex • Rounded iliac wings • Underdeveloped acetabula • Dysplastic capital femoral epiphyses • Coxa valga • Genu valgum • Ankle valgus 8 year old Morquio A Image courtesy of Ralph Lachman, MD 6 year old Morquio A Image courtesy of Klane White, MD White, Curr Orthop Prac, 2012
Thorax: Normal Image courtesy of Ralph Lachman, MD
Thorax: Dysostosis multiplex • Paddle-shaped ribs • Pectus carinatum • Short, thick clavices 8 year old Morquio A Image courtesy of Christina Lampe, MD
Hands: Normal Image courtesy of Ralph Lachman, MD
Hands: Dysostosis multiplex • Short, broad metacarpals • Proximal metacarpal rounding • Hypoplastic carpal ossification 8 year old Morquio A Image courtesy of Ralph Lachman, MD
Short stature is a characteristic feature of Morquio A Growth retardation in Morquio A • 71% of Morquio A subjects ≤ 18 years are below 3rd percentile in height • Majority of adults are < 120 cm in height n=325 Morquio A subjects MorCAP baseline data Harmatz et al, Mol Genet Metab, 2013; BioMarin data on file
Short stature is a characteristic feature of Morquio A Growth retardation in Morquio A Montano et al, J Inherit Metab Dis, 2007 International Morquio A registry
Joint abnormalities are common in Morquio A patients • Joint instability • floppy wrists with weak grip and loss of fine motor skills • exacerbates knee valgus and gait abnormalities • Subluxations of the hip and atlantoaxial joints are common • Joint degeneration due to bone defects, cartilage deterioration and altered mechanics • Joint pain Atinga et al, J Bone Joint Surg Br, 2008 Harmatz et al, Mol Genet Metab, 2013; Aslam et al, JIMD Rep, 2013; Tomatsu et al, CurrPharmBiotechnol, 2011; Montano et al, J Inherit MetabDis, 2007
Hand function is compromised • A study of 10 Morquio A patients (Aslam et al, 2012) revealed: • Wrist instability in all subjects • Average difference of 93 between active and passive ROM at wrist joint • Reduced hand grip strength in all subjects • Difficulties with tasks requiring strength, e.g. lifting heavy objects and pouring from a bottle • Of the 153 subjects ≥ 12 years of age in the MorCAP baseline study (Harmatz et al, 2013): • 30% could not cut their fingernails • 22% could not tuck in shirts • 22% were unable to open jars • 20% were unable to tie shoelaces Hand dysfunction contributes significantly to difficulties with activities of daily living Aslam et al, JIMD Rep, 2013; Harmatz et al, Mol Genet Metab, 2013; BioMarin data on file
Abnormal gait results from bone and joint defects • A study of 9 children with Morquio (subtype not specified) with no previous lower extremity surgery revealed a consistent gait pattern: • Slower walking speed, reduced cadence and reduced stride length vs normal • Trunk, pelvis, hip: increased forward tilt of trunk and pelvis, increased hip flexion • Knee: increased knee flexion, genu valgus, and external tibial torsion; dynamic knee varus-valgus joint laxity • Joint moments and power: reduced hip and ankle joint moments, reduced power generation Embed Dawn video (Youtube) http://www.youtube.com/watch?v=ugeVScsV0oM Dhawale et al, J PediatrOrthop B, 2012
Orthopedic management of the spine, hips and lower extremities is essential for optimal patient outcomes Cervical instability, spinal stenosis and spinal cord compression are common in Morquio A. Early diagnosis and timely intervention can reduce the risk of myelopathy, quadriparesis and death. At 4 years old At 7 years old Progressive genuvalgum and hip deformity in Morquio A. Surgical correction can improve mechanics, increase walking ability and endurance, reduce pain, and delay onset of arthritis. Solanki et al, J Inherit Metab Dis, 2013 Radiographs from Dhawale et al, J PediatrOrthop B, 2012 Solanki et al, J Inherit MetabDis, 2013; Dhawale et al, J PediatrOrthop B, 2012; White, Rheumatology, 2011; White, CurrOrthopPrac, 2012
Regular assessments of the spine are recommended for improved patient outcomes Solanki et al, J Inherit MetabDis, 2013
Surgical interventions • Indications include: • Neurological deficits + instability • Cord compression with signal change on MRI • Cervical spine: • Posterior fusion for C1-C2 subluxation and instability, often with posterior occipito-cervical fixation • If subluxation is irreducible and cord compression is present, decompression + fusion is indicated • Prophylatic fusion recommended by some • Thoracolumbarkyphosis: • Decompression, segmental instrumentation and fusion • Anterior discectomy and fusion strongly recommended to augment posterior fusion in cases of rigid kyphosis Ain et al, Spine, 2006 Image courtesy of Klane White, MD White, Curr Orthop Prac, 2012 Solanki et al, J Inherit MetabDis, 2013; White, CurrOrthopPrac, 2012; Ain et al, Spine (Phila PA 1976), 2006; Ransford et al, J Bone Joint Surg Br, 1996; Lipson, J Bone Joint Surg Am, 1977
Outcomes of spine surgery • Short-term post-operative outcomes generally good • Possible post-surgical complications: • Late instability below fusion site may necessitate multiple fusions • Halo pin tract infection → Long-term monitoring is important • Long-term outcomes beyond 5 years are less known – few studies Morquio patient 26 years post-surgery: complete resolution of quadriparesis achieved and neurological function maintained 26 years after C1-C2 decompression and stabilization Image courtesy of Klane White, MD White, J Bone Joint Surg Am, 2009 Solanki et al, J Inherit Metab Dis, 2013; White, J Bone Joint Surg Am, 2009; Ain et al, Spine (Phila PA 1976), 2006; Dalvie et al, J Pediatr Orthop B, 2001; Holte et al, Neuro-Orthopedics,1994; Houten et al, Pediatr Neurosurg, 2011; Lipson, J Bone Joint Surg Am, 1977; Ransford et al, J Bone Joint Surg Br, 1996; Stevens et al, J Bone Joint Surg Br 1991; Svensson and Aaro, Act Orthop Scand, 1988.
Regular assessments of the hips and lower extremities are recommended for optimal outcomes White, Rheumatology, 2011
Hip deformity correction and outcomes • Pelvic osteotomy + femoral osteotomy • Hip subluxation may recur • Shelf acetabuloplasty + femoral varus derotation osteotomy (VDRO) reported to yield good outcomes with no recurrent hip subluxation • Total hip arthroplasty Morquio A patient with hip subluxation: (A) At 12.5 years underwent Pemberton osteotomy + VDRO. (B) At 16 years, hip subluxation recurred. (C) At 18 years, hips well located 2 years post-shelf acetabuloplasty Morquio adult: satisfactory bilateral hip replacement, 7 year followup Dhawale et al, J Pediatr Orthop, 2012 Lewis et al, J Bone Joint Surg Br, 2010 Dhawale et al, J PediatrOrthop, 2012; Tassanari et al, ChirOrganiMov, 2008; Lewis et al, J Bone Joint Surg Br, 2010; White, CurrOrthopPrac, 2012
Knee deformity correction and outcomes • Guided growth for younger patients with mild to moderate genu valgum • Osteotomy for patients with limited growth potential and severe genu valgum • Recurrence after genu valgum correction is common • Total knee arthroplasty for patients with advanced arthrosis Hemiepiphysiodesis (F) of proximal tibia and distal femur with 8 plates in 10 year old Morquio A patient. (G) Maintenance of correction 1 year after removal of 8 plates, at age 13 years. Patient also underwent guided growth for ankle valgus. Morquio A adult, 4 years after total knee arthroplasty de Waal Malefijt et al. Arch Orthop Trauma Surg, 2000 Dhawale et al, J Pediatr Orthop, 2012 Dhawale et al, J PediatrOrthop, 2012; de Waal Malefijt et al. Arch Orthop Trauma Surg, 2000; Atinga et al, J Bone Joint Surg Br, 2008; White, CurrOrthopPrac, 2012
Airway and anesthetic management of Morquio A patients presenting for surgery is challenging • Morquio A patients are at high risk of anesthesia-related morbidity and mortality due to: • Cervical instability and myelopathy • Compromised respiratory function • Upper and lower airway obstruction • Restrictive lung disease • Cardiac abnormalities • Any elective surgery requires: • Thorough pre-operative ENT, pulmonary and cardiac evaluations • Pre-operative radiological assessment of the cervical spine • Skilled personnel in airway management • Spectrum of airway management equipment • Morquio A patients should be managed by experienced anesthesiologists at centers familiar with MPS disorders Theroux et al, PaediatrAnaesth, 2012; Solanki et al, J Inherit MetabDis, 2013; Walker et al, J Inherit MetabDis, 2013; McLaughlin et al, BMC Anesthesiol, 2010; Morgan et al, PaediatrAnaesth, 2002; Shinhar et al, Arch Otolaryngol Head Neck Surg, 2004; Belani et al, J PedSurg, 1993; Walker et al, Anaesthesia, 1994
Non-surgical interventions • Physical therapy • Walker/wheelchair use • Pain management • MorCAP baseline data (Harmatz et al, 2013) revealed: • 49% of 300 Morquio A subjects required wheelchairs (mean age= 14.5 years) • 26% of 298 Morquio A subjects used walking aids (mean age= 14.5 years) Harmatz et al, Mol Genet Metab, 2013