Download
1 / 67
960 likes | 2.33k Vues
CT of the Chest. Dorith Shaham, M.D. Department of Radiology Hadassah Medical Center. Indications for Chest CT. To evaluate abnormalities shown on CXR To demonstrate or exclude a suspected CXR abnormality To demonstrate an abnormality in a patient with a normal CXR. Types of Chest CT.

E N D
CT of the Chest Dorith Shaham, M.D. Department of Radiology Hadassah Medical Center
Indications for Chest CT • To evaluate abnormalities shown on CXR • To demonstrate or exclude a suspected CXR abnormality • To demonstrate an abnormality in a patient with a normal CXR
Types of Chest CT • Standard chest CT • Without IV contrast • With IV contrast • CT-angiography • PCTA (r/o PE) • Coronary CTA • HRCT • CT-guided intervention • Biopsy • Pleural drainage • Low-dose CT
IV contrast • Not used for pulmonary parenchimal abnormalities • Inherent high contrast • Always used for CT-angiography • May be used for evaluation of • Mediastinum • Hilum • Pleura
Metastatic Lung Ca (Adenocarcinoma)Rt. Hilar mass and small pleural effusion Without IV contrast
Anterior Mediastinal Mass : Germ cell tumor Without IV contrast With IV contrast
Chest CT with IV contrast Venous collaterals Thrombus SVC syndrome
Pulmonary Embolism:Imaging Modalities • Chest X-ray • V/Q scan • Computed tomography • Helical (spiral) CT • MRI • Pulmonary angiography: the “gold standard”
Ventilation-perfusion (V/Q) scan • Perfusion scan: distribution of blood flow • Macroaggregated human serum albumin (10-100 micron) labeled with Tc-99m • Ventilation scan: distribution of alveolar ventilation • Radioactive inert gas: X-133 • V/Q mismatch: abnormal perfusion and normal ventilation
Interpretation of V/Q scanning • Probability stratification approach (based on the assumption that the only reason for performing a V/Q scan is to diagnose PE): • High probability • Intermediate probability/ indeterminate • Low probability • Normal
Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) • Multi-institutional study conducted in the mid-80’s, • Purpose: to determine the sensitivity and specificity of V/Q scan compared with pulmonary angiogram • 933 patients with suspected PE • 931 had V/Q scan • 755 had pulmonary angiography • Study patients were followed clinically for 1 Y
PIOPED STUDY • High sensitivity of V/Q scan: 98% of patients with PE had abnormal scans (low, intermediate or high probability) • Low specificity: 10% • Non-diagnostic V/Q scans: 72%
CTPA • Direct visualization of clot • Imaging of associated findings • Pulmonary infarction • Pleural effusion • Imaging of alternative diagnosis
Pulmonary Embolism with Infarction Atelectasis Infarction
Combined PCTA/CTV • No additional contrast injection • Rapid examination • Imaging of portions of the deep venous system that are inadequately imaged by Duplex (pelvic veins, adductor canal)
PIOPED II • To determine the sensitivity, specificity, positive/negative predictive value of spiral CT for the diagnosis of PE. • Reference for PE: various combinations of • V/P scan • Venous U/S • Pulmonary angiography • Contrast venography
PIOPED II • 824 patients with suspected PE • CTPA alone: • Sensitivity: 83% • Specificity: 96% • PPV: 96% (concordant high/low clinical probability), 92% (intermediate clinical probability)
PIOPED II • Combined CTPA + CTV: • Sensitivity: 90% • Specificity: 95% • Additional testing is necessary when clinical probability is inconsistent with imaging results N Engl J Med 2006;354:2317-27
Intramural hematoma Pericardial effusion Small right pleural effusion
Coarctation of the aorta with enlarged internal mammary arteries
HRCT: Technique • Narrow slice width • “Bone” reconstruction algorithm • Small field of view
HRCT: Ground glass opacity Chest CT HRCT
HRCT: scanning protocols • 1-mm slices every 10-mm/ Contiguous 1-mm slices • Supine/ Prone • Full inspiration/ Expiration
HRCT: patterns of lung disease • Reticular and short linear • Nodular • Increased lung opacity (“ground glass”) • Decreased lung density • Cysts • Emphysema • Bronchiectasis
CT vs. HRCT Sarcoidosis Multiple tiny perilymphatic nodules
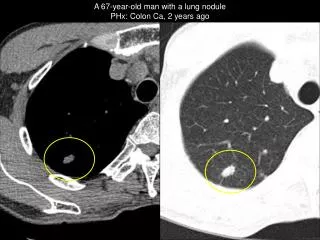
Indications • Evaluation of • Solitary pulmonary nodule • Multiple pulmonary nodules • Mediastinal/hilar masses/lymphadenopathy • Chest wall masses • Retrieval of organisms from infectious lung lesions • Staging of tumors (lung cancer, extrathoracic)
Contraindications • An uncooperative patient • Bleeding diathesis • INR>1.3 • Platelet count<50,000 mm3 • Severe underlying lung disease • emphysema • Intractable cough
Image Guidance • CT • Fluoroscopy • visualization in 2 projections • Ultrasound • chest wall • pleura • anterior mediastinum • lung periphery
Advantages of CT-guided Biopsy • Needle path that avoids • aerated lung • fissures • large vessels • bullae • vital cardiovascular structures • Differentiation of necrotic vs. viable portions of tumor • I.V. contrast