Download

1 / 23
310 likes | 810 Vues
Coronary CT Angiography. Intern 柳復威. Udo Hoffmann, Maros Ferencik, Ricardo C. Cury, and Antonio J. Pena Coronary CT Angiography J Nucl Med May 1 2006 47: 797-806.

E N D
Coronary CT Angiography Intern 柳復威
Udo Hoffmann, Maros Ferencik, Ricardo C. Cury, and Antonio J. Pena Coronary CT AngiographyJ Nucl Med May 1 2006 47: 797-806.
64-slice coronary CT angiography is highly accurate for the exclusion of significant coronary artery stenosis (>50% luminal narrowing) • with negative predictive values of 97%–100%, in comparison with invasive selective coronary angiography.
INTRODUCTION • patient preparation • image acquisition • evaluation techniques
patient preparation Image quality improved at low heart rates (<65 beats per minute) 1. the inspirational breath hold (-6beats/min) 2. oral ß-blocker (50—100mg oral or 5–20 mg i.v. metoprolol) 3. combination (-11beats/min) 4. short-acting nitroglycerin (selective coronary angiography ) Supine position Sedation
image acquisition • A low-energy topogram determination of the adequate initiation of the coronary CTA image acquisition to ensure homogeneous contrast enhancement of the entire coronary artery tree • Two techniques: 1. the timing bolus technique 2. the bolus tracking technique • CT volume dataset
The minimal equipment requirement for state-of-the-art coronary CTA is a 16-slice scanner. However, 40- or 64-slice MDCT scanners are recommended, as they increasethe volume coverage and permit reduction of the scan time and the amount of contrast agent.
Radiation exposure • 64-slice MDCT:11~22mSv (ECG-controlled dose modulation is 7–11mSv) • invasive selective coronary angiography: 2.5–5mSv, • nuclear perfusion imaging with SPECT: 15~20mSv
Image evaluation • multiplanar reformatted (MPR) images For the confirmation of pathologic findings in the long and short axes of the vessel. • sliding thin-slab MIP (STS-MIP) images enhance the visualization of coronary artery stenosis in a long-axis view of the vessel if narrowing is caused by noncalcified atherosclerotic plaque
Artifact • Motion Artifacts:occur at high rates and most often in the midsegment of the right coronary artery • Misalignment and Slab Artifacts:high heart rates, heart rate variability, and the presence of irregular or ectopic heart beats (e.g. PVC) • Blooming Artifacts:High-attenuation structures, such as calcified plaques or stents, appear enlarged (or bloomed) because of partial volume averaging effects and obscure the adjacent coronary lumen, the main cause of false-positive results in coronary CTA because of overestimation of the degree of stenosis
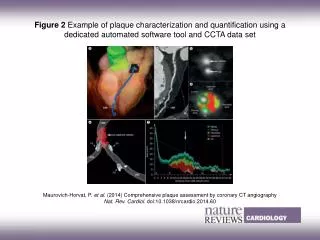
FINDINGS AND POTENTIAL CLINICAL APPLICATIONS • Detection of Significant Coronary Artery Stenosis moderate sensitivity (about 80%) and excellent specificity (about 90%) • Detection and Characterization of Coronary Atherosclerotic Plaque 1. detects calcified or mixed plaque with sensitivities and specificities above 90%. 2. the detection of noncalcified plaques, with sensitivities and specificities ranging from 60% to 85%, but has the potential to further stratify noncalcified plaque into fibrous plaque and lipid-rich plaque 3. smaller plaques (<0.5 mm) are not detected
Potential Clinical Applications limitation • Data based on single-center, multicenter trials and studies with intermediate-risk populations are warranted • a very specific subset of symptomatic middle-aged white men who had a high prevalence of CAD Other potential applications • coronary CTA is to improve the triage and management of patients with acute chest pain. • preoperative risk • patency of stents placed in the left main coronary artery • bypass patency
CONCLUSION • Severe coronary calcification remains the major limiting factor in coronary CTA. • The high negative predictive value of 64-slice MDCT, relative to invasive selective coronary angiography, can rule out the presence of hemodynamically significant CAD. • Although data on clinical utility, cost, and cost-effectiveness are not yet available, coronary CTA may improve the management of patients with an intermediate probability of CAD and patients with acute chest pain.