Download
1 / 13
160 likes | 428 Vues
CT perfusion and CT angiography before thrombolysis in acute stroke. Kinga Pozsár , Géza Szilágyi PhD*, Gábor Forrai PhD National Health Center, Radiology Department * Neurology Department , Budapest Hungary. CLINICAL PROTOCOL

E N D
CT perfusion and CT angiography beforethrombolysisinacute stroke Kinga Pozsár , Géza Szilágyi PhD*, Gábor Forrai PhD National Health Center, RadiologyDepartment *NeurologyDepartment, Budapest Hungary
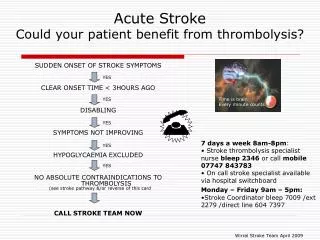
CLINICAL PROTOCOL 2007- 110 patientswithintravenousthrombolysis, 2007 AHA, 2009 ESO guidelines NECT examination PATIENT EmergencyDepartment: physical, neurologicalexamination, laboratorytests no CTA,CTP CT positive (hemorrhage, tumour, stb.) over3 (4.5) hours within 3 (4.5) hours yes MCA or T occlusionor BA occlusion MCA or T occlusionor BA occlusion Admissiontoneurologydepartmentorotherdepartment no yes no yes Admissiontoneurologydepartmentorotherdepartment IVT-IAT bridging IVT IAT
RADIOLOGICAL PROTOCOL • Unenhanced CT examination • -exlusion of hemorrhage • Perfusion CT examination • -strokeradiologicaldiagnosis • -therapeuticplan (perfusiondamagedarea’ssize and viablearea’sproportion) • CT angiography • -site of theocclusion • -evaluation of thecarotidsystem ( intraarteriallysis) • Contrastenhanced CT examination • - Contraindication of thrombolysis (luxusperfusion, otherpathologicalenhancedareas-tumours) • Followup CT examination (24, 48 hours) • - hemorrhagiccomplications • - size of finallydamagedarea
DATABASE • 30 patients17 females, 13 malesAge 69.8±12.9 years • Time (CT) 107.2±25,1 minutes • Time (thrombolysis) 153.8±32,1 minutes • Riskfactors • Hypertension 82% • Ischaemicheartdisease45% • Atrialfibrillation 36% • Stroke 22% • DM 18% • GroupsbasedonCTA • Main arteryocclusion ICA or T occlusion • MCA primarybranchocclusion • MCA secondary-third-branchocclusion
AIMS • Weexaminedtheperfusiondamage, penumbra and supposedlydamagedarea’ssizeandproportionfurthermoreonfollowup CT weexaminedsaved and finallydamagedarea’ssizeandproportionineachgroup • Penumbra – perfusionmismatch (MTT-CBV) MTT:7-8 sec, CBV:3ml/100g braintissue • Supposedlyfinallydamagedarea – CBV • Finallydamagedarea-followup CT hypodensity • Cooperatingwithneurologistswecomparedthe CT studyresultswith clinicalimprovement -NIHSS (National Institutes of Health Stroke Scale) -mRankinscale • Efficiency of intravenousthrombolysisfromclinical and radiologicalpoint of view
ICA OCCLUSION MTT Followup CT CBF CBV CTA
SECONDARY BRANCH OCCLUSION MTT CBF Followup CT CTA CBV
PERFUSION CT- RESULTS ICA, T occlusion MCA primarybranchocclusion Secondary branchocclusion CBV MTT Penumbra Infarct Intherelevantslices Savedarea
PERFUSION CT- RESULTS ICA, T occlusion ICA, T occlusion CBV Damagedarea Penumbra Savedarea MCA primary branch occlusion MCA primary branch occlusion CBV Damaged area Penumbra Saved area MCA secondary branch occlusion MCA secondary branch occlusion Damaged area CBV Penumbra Saved area
NEUROLOGICAL OUTCOME ICA, T occlusion MCA primary branch occlusion Secondary branch occlusion NHISS before NHISS 7 days later mRankin 7 days later Allpatientswithsecondarybranchocclusionwenthome, 8patinetsgottotherehabilitation center, 9 patientgottothechronic center, 3 patientsdied
CT PERFUSION-DIAGNOSTIC ROLE CBV CTA MTT Young patientwithmildhemisymptoms Perfusiondamagedareainbasalganglions in PCA territory Smallpartialbasilarthrombosis Therapeuticplan IA lysis CTA
SUMMARY CTP and CTA studiesareusefulforseveralreasons quick and easilyavailable Diagnosticrole (stroke radiologicaldiagnosis-differentialdiagnosis) Therapeuticrole (settinguptherapeuticplan and foreseeingthetherapeuticefficiency) Considerations - Patientsarrivingwithin 2 hoursatthehospitalhaveremarkablepenumbra - A major part of penumbracan be savedperformingintravenouslysis - Incase of main arteryocclusionnearlythewholepenumbracan be savedwithin 3 hours - Incase of secondarybranchocclusiontheintravenouslysisresultsinoptimalfunctionaloutcome, howeverthewholepenumbra is notsaved IF THE CT PROTOCOL IS NOT ACCURATE FOR ANY REASON MRI EXAMINATION IS NECESSARY