Download
1 / 25
250 likes | 388 Vues
CONSEQUENCES OF AND POLICY RESPONSES TO THE TOBACCO EPIDEMIC IN SOUTH-EAST EUROPE. Ivana Bozicevic School of Public Health, Croatia.

E N D
CONSEQUENCES OF AND POLICY RESPONSES TO THE TOBACCO EPIDEMIC IN SOUTH-EAST EUROPE Ivana Bozicevic School of Public Health, Croatia
The studyhas been carried out in 7 countries of south-east Europe (SEE)– Albania, Bosnia and Herzegovina, Bulgaria, Croatia, Macedonia, Romania, Yugoslavia (Serbia and Montenegro) • Funded by the Open Society Institute
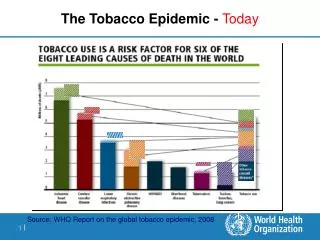
Aims of the project • To collect and present data on a range of issues relevant for tobacco control policies in south-east European countries: - data on tobacco consumption and prevalence of smoking in youth and adults • burden of disease related to tobacco • tobacco industry activities and economics related to tobacco (tax policies, smuggling of tobacco products) • tobacco control laws and regulations; tobacco control programmes • NGOs that are active in tobacco control
Some characteristics of the SEE region • The total population of the seven countries is around 44 million • In 2001 GDP ranged from US$ 1180 in B&H to US$ 4566 in Croatia • In 2001, the GDP in SEE countries was 88% of its levels in 1990. In CEE countries it was 119% • Unemployment rates: from 9.6% in Romania to 43% in B&H
Important issue: Quality of health indicators • The quality of information on health indicators during 1990s for countries of ex-YUwas inadequate, and for some countries (B&H, Yugoslavia) most health indicators in the WHO Health for All Database have simply not been available since 1991 • There has also been research on the impact of the socio-economic transition and the wars on the population health status, particularly in countries of ex-Yugoslavia
Prevalence of smoking (in %) Youth Adults Males Females Males Females Albania 49 14 38 19 B&H 53 47 60 Bulgaria 35 38 38.4 16.7 Croatia 31 25 34.1 26.6 Macedonia 22 18 No data Romania39 10 7239 Yugoslavia 22.4 24.2 56 44
Smoking among physicians • In Macedonia 40% of male physicians and 32% of female physicians smoke • In Bosnia and Herzegovina53% of physicianssmoke • By information provided by the Serbian Ministry of Health, 37% of physicians and 52% of nurses at the Clinical Hospital Serbia smoke
Surveys that aimed to assess prevalence of tobacco consumption used different methods and population groups • The best quality surveys were carried out in Bulgaria and Albania and both estimated smoking prevalence in males and females to be the highest in those younger than 35 • Per capita consumption of cigarettes in SEE: In 2000 onaverage 2335 cigarettes - that is9.6% higherthan in the CEE countriesand 41.3% higher than in the EU countries
Standardised lung cancer incidence rates, all ages, per 100,000 Males Females Albania79.2412.95 B&H81.2413.21 Bulgaria48.917.96 Croatia82.4711.81 Macedonia46.918.08 Romania50.668.31 Yugoslavia80.8913.79 Eastern Europe 69.708.77 Western Europe53.2110.68 Estimates for 2000, International Agency for Research on Cancer
Standardised death rates from smoking related causes, 2000 data Males Females Albania500.36292.84 Bulgaria569.56350.03 Croatia649.01349.09 Macedonia461.32286.16 Romania650.74414.70 CEE556.56300.27 EU 349.29164.29 WHO Health for All Database. Kopenhagen. 2002
Overall mortality caused by tobacco in males in the SEE countries for which data are available is 62.1% higher than the EU average, whereas in females it is on average more than twice higher compared with the EU countries • We have considered only the direct health impacts of smoking. Indirect impacts through involuntary exposure to passive smoking are also considerable particularly given the high rates of smoking in public places. • A problem with analyses of mortality data is that estimates ofpopulation number for countries of ex-Yugoslavia have limited accuracy because of large-scale population movements during the wars in 1990s
Economics related to tobacco and tobacco industry • TTC started to invest in previously state-owned tobacco monopolies in countries of south-east Europe later than in CEE and FSU countries because of conflicts in Balkans • They particularly dominate Romanian market and are expressing interests in purchasing tobacco companies in the rest of the countries (B&H, Croatia and Serbia) • BAT is negotiating the move of its regional office from Budapest to Zagreb during 2003 and plans to start serious negotiations to acquire the Rovinj tobacco company.
Excise tax rate (as % of retail price) • Albania 38 • B&H 35 • Bulgaria 37 • Croatia 50 • Macedonia 35 • Romania 38 • Yugoslavia 40
Cigarettes are the most expensive in Croatia and the cheapest in Bosnia and Herzegovina. The prices of the cheapest domestic cigarettes range from 0.3 to 1.4 US$. The price of Marlboro ranges from US$1 to US$2 • Cigarettes are affordable, particularly if taken into account that smuggled cigarettes can be bought even cheaper • Only Romania earmarks tax from tobacco for health care purposes
Smuggling … is the major characteristic of tobacco market in SEE • It is estimated that up to 25% of the cigarette consumption in Croatia comprises of smuggled cigarettes and 38% in Bulgaria, 36.5% in Yugoslavia, 40% in Macedonia, 47% in B&H and even 80% in Albania
The Annual Report of the Croatian Ministry of Finance for 2000 noted «With regard to the fact that excise taxes on tobacco products at the end of 1999 grew on average by almost 19% and again from July 1, 2000 by an additional 10.5%, the increase in revenue (only 5.6%) was definitely below all expectations. The answer to such a poor collection of revenues is in the fact that the number of taxable cigarettes packets in 2000 dropped by almost 20% in comparison with 1999. This decrease cannot be justified by the decrease in the number of smokers or reduced smoking in Croatia. The reason for such decrease in taxed cigarettes quantities is for the largest part the increase in the informal cigarette market"
In survey carried out in 2002 by the Croatian leading independent journal Nacional, current and ex Croatian ministers, leading politicians and economists identified tobacco company Rovinj as the most powerful business company in terms of the influence in defining and creating Croatian economic policy, particularly related to tax policy, customs administration and subventions. It was estimated in 2002 that revenues lost due to cigarette smuggling were aroundUS$ 57,143.000 in Croatia.
The countries of SEE have achieved certain progress in tobacco control programmes at the end of 1990s and beginning of 2000s, particularly in terms of legislation. • They share some common characteristics which have influenced directly or indirectly development of their tobacco control policies: less developedpublic health advocacy, weaknesses of the judiciary systems, limited capacities of law enforcement, presence of corruption and organised crime
Main findings • Burden of disease related to tobacco is already large, per capita cigarette consumption is high, prevalence of smoking high in youth and younger adults which means that tobacco epidemic will continue to pose a major threat to health of populations • The problem is particularly acute in Croatia, B&H and Albania, suggesting that the tobacco epidemic in these countries is longer-established. This is supported by high smoking rates in Croatia, B&H and Albania, in both adults and youth • In Yugoslavia and Macedonia, lung cancer mortality is rising rapidly suggesting that the tobacco epidemic is at an earlier stage and still growing
All the south-east European countries have intersectoral coordinating committees on tobacco control at ministries of health but national action plans against tobacco have not been developed, except in Bulgaria
Conclusions There are numerous promising initiatives and efforts initiated by the ministries of health, academic institutions and and NGOs that will certainly contribute to development of more comprehensive tobacco control policies
Need for… further intersectoral actions • Development of national action plans on tobacco control - consisting of specific targets, processes that enable reaching themand roles of key stakeholders) • Increase in tobacco taxes • Adoption and enforcement of regulatory changes • Actions against smuggling • Defining the role that health services can play in the primary and secondary prevention of tobacco-related diseases
If health policies against smoking are to be properly targeted we also need... • Regular collection of data on prevalence of smoking (according to socio-economic status, urban/rural residence), determinants of smoking • More research on burden of disease related to smoking, health care costs imposed by smokers • Provision of information to smokers and the general public on dangers of tobacco usage • Death certificates should contain the information on the past smoking status and basic socio-economic data
The crucial issue in tobacco control remains building knowledge, expert and regulatory capacities which are necessary for achieving better outcomes and sustainability of such efforts