Download
1 / 46
460 likes | 467 Vues
Management of non neoplastic portal vein thrombosis in the setting of liver transplantation (LT). Journal club 18/02/2019 Specializzanda: Dott.ssa C. Chialà. Definition.

E N D
Management of non neoplastic portal vein thrombosis in the setting of liver transplantation (LT) Journal club 18/02/2019 Specializzanda: Dott.ssa C. Chialà
Definition Portal vein thrombosis (PVT) refers to the thrombotic occupation in the portal lumen, which can affect the intrahepatic and the extrahepatic venous tracts.
Incidence and prevalence in the setting of LT • Few data on incidence: Francoz et al. (Gut 2005) found that of 251 patients with cirrhosis listed for LT, 17 (7,4%) developed de novo PVT after the initial evaluation during a mean of 12 months follow-up. • In a review (Transplantation 2012) collecting data on 41 studies, of 25753 LTs 2004 were performed in patients with PVT. The mean of the reported data on prevalence is 9,7% ± 4,5%. Francoz C et al., Splanchnic vein thrombosis in candidates for liver transplantation: usefulness of screening and anticoagulation. Gut 2005; 54:691. Rodriguez-Castro K et al., Management of nonneoplastic portal vein thrombosis in the setting of liver transplantation: a systematic review, Transplantation 2012; 94: 1145-1153.
Risk factors for pvt in cirrhotic patients undergoing lt • Cirrhosis as a prothrombotic condition (hypercoagulable state associated with low portal vein flow) • HCC (Rule out neoplastic PVT!) • Underlying genetic thrombophilic conditions (e.g. prothrombin gene mutations) • Male sex • Previous treatment of portal hypertension-related bleeding (sclerotherapy, TIPS) • Worsening liver disease (Child C) • Diagnosis of fatty liver disease, alcoholic liver disease or cryptogenic cirrhosis • Diabetes mellitus • Higher body mass index Rodriguez-Castro K et al., Management of nonneoplastic portal vein thrombosis in the setting of liver transplantation: a systematic review, Transplantation 2012; 94: 1145-1153. Ghabril M et al., Portal vein thrombosis is a risk factor for poor early outcomes after liver transplantation: analysis of risk factors and outcomes for portal vein thrombosis in waitlisted patients, Transplantation 2016; 100: 126-133.
Risk factors for pvt in cirrhotic patients undergoing lt The presence of at least one risk factor, including male sex, previous treatment of portal hypertension, Child C class severity of liver disease, and the presence of alcoholic liver disease, increases the rate of PVT from 6,6% (absence of risk factors) to 12,5% (p<0,013). Possible role of NSBB as risk factor for PVT (?) Yerdel MA et al., Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management and outcome, Transplantation 2000; 69: 1873.
Classification of pvt Yerdel MA et al., Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management and outcome, Transplantation 2000; 69: 1873.
Classification of pvt Yerdel classification is considered the most adequate in the setting of LT because it best correlates thrombosis extension with the feasible surgical techniques and outcome. Yerdel MA et al., Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management and outcome, Transplantation 2000; 69: 1873.
Classification of pvt Yerdel classification is considered the most adequate in the setting of LT because it best correlates thrombosis extension with the feasible surgical techniques and outcome. Yerdel MA et al., Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management and outcome, Transplantation 2000; 69: 1873.
PVT at listing is not associated with lower transplant rates, or delisting for death, or deterioration; it is indipendently associated with increased 90-day mortality (p<0,001) and graft failure (p<0,001). Ghabril M et al., Portal vein thrombosis is a risk factor for poor early outcomes after liver transplantation: analysis of risk factors and outcomes for portal vein thrombosis in waitlisted patients, Transplantation 2016; 100: 126-133
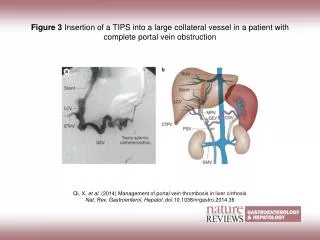
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION For patients with PVT awaiting LT, treatment is fundamental for two main reasons: Avoid progression of thrombosis, that could represent a risk of delisting, if thrombosis goes beyond surgical feasibility. Allow portal flow to the graft to be restored through conventional end-to-end PV anastomosis, associated with a better LT outcome in comparison with those transplants in which other surgical approaches for PV vascularization are needed, Chen H et al., Nontumoral portal vein thrombosis in patients awaiting liver transplantation. Liver transplantation 2016; 22:352–365.
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION • Anticoagulation in the setting of PVT in LT candidates is recommended. • Another option is the intravascular stenting of the obstructed portal vein via either a transhepatic or sometimes transplenic approach, often in combination with mechanical or lytic thrombectomy. • LIMITATIONS: • Technically demanding procedure, only available at centers with significant expertise • Invasive • Alters anatomy permanently • Risk of adverse events (HE for TIPS) • Unclear if anticoagulation is however needed after these procedures • No randomized trials available
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION • Anticoagulation in the setting of PVT in LT candidates is recommended.
Anticoagulation in PVT in cirrhosis is effective and safe: • 16 studies included, 430 treated patients • No lethal complications recorded • Anticoagulation-related bleeding : 3,3% (0-18) • Portal vein recanalization: 66,6% (37-93) • Complete portal vein recanalization: 41,5% (0-75) • Complete recanalization significantly higher in anticoagulation group than in non-anticoagulation group (p:0,0004)
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION Anticoagulation in the setting of PVT in LT candidates is recommended. Questions: Bleeding risk? Which anticoagulant? LMWH? VKA? DOACs? Timing: immediately or after variceal treatment? Ligation/betablockers
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION Anticoagulation in the setting of PVT in LT candidates is recommended. Questions: Bleeding risk? Which anticoagulant? LMWH? VKA? DOACs? Timing: immediately or after variceal treatment? Ligation/betablockers
Chronic liver disease, particularly in the advanced or decompensated stages, has historically been regarded as an example of an acquired bleeding diathesis: • Abnormalities in basic conventional laboratory tests of coagulation such as the prothrombin time (PT), activated partial thromboplastin time (aPTT) and international normalized ratio (INR); • Thrombocytopenia of liver disease.
Northup P and Reutemann B, Management of coagulation and anticoagulation in liver transplantation candidates, Liver transplantation 2018 Aug;24(8):1119-1132.
Neither PT nor INR accurately reflects the in vivo coagulation status of patients with liver disease because these tests only measure the levels of procoagulant proteins and fail to account for the concurrent alterations in anticoagulant proteins or platelets that are known to occur in these patients. Many studies has disproven the role of elevated INR as an indicator of bleeding risk in the setting of multiple invasive procedures: paracentesis, liver biopsy, arterial needle punctures during cardiac catheterization, and even in LT. 1. Grabau CM et al., Performance standards for therapeutic abdominal paracentesis. Hepatology 2004;40:484-488. 2. Segal JB et al., Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures: an evidence-based review. Transfusion 2005;45:1413-1425. 3. Jeffers L et al., Safety and efficacy of recombinant factor VIIa in patients with liver disease undergoing laparoscopic liver biopsy. Gastroenterology 2002;123:118-126. 4. Townsend JC et al., Usefulness of international normalized ratio to predict bleeding complications in patients with end-stage liver disease who undergo cardiac catheterization. Am J Cardiol 2012;110:1062-1065. 5. Planinsic RM et al., Safety and efficacy of a single bolus administration of recombinant factor VIIa in liver transplantation due to chronic liver disease. Liver Transpl 2005;11:895-900.
INRis not predictive of bleeding risk in cirrhosis patients, except perhaps at the extreme range of elevations, and in these patients SHOUL NOT BE USED AS A MEASURE OF BLEEDING RISK! • Prophylactic protocol transfusions including large doses of fresh frozen plasma (FFP) to «correct» the INR are INEFFECTIVE AND EVEN POTENTIALLY HARMFUL INTERVENTIONS based on an outdated understanding of hemostasis in cirrhosis. • The modern understanding of hemostasis in cirrhosis involves a rebalance of hemostasis with a tenuous equilibrium between clotting and bleeding , of which the clinician should be aware.
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION Anticoagulation in the setting of PVT in LT candidates is recommended. Questions: Bleeding risk? Which anticoagulant? LMWH? VKA? DOACs? Timing: immediately or after variceal treatment? Ligation/betablockers
Which anticoagulant? • VKA are not ideal for medical therapeutic anticoagulation in this population: • INR system is disrupted in liver disease patients and is elevated at baseline in most cirrhotic (difficulty in monitoring VKA activity) • VKA decrease also protein C activity (potential paradoxical thrombophilia) • Narrow therapeutic window Lee SJ et al., The safety and efficacy of vitamin K antagonist in patients with atrial fibrillation and liver cirrhosis. Int J Cardiol 2015;180:185-191.
Which anticoagulant? • LMWHs are the most tested anticoagulants in the cirrhosis population. • PROs: • Shorter half-life compared with VKA (easier management) • Significant accumulated safety and efficacy data1,2 • CONs: • Injectable-only formulation (difficult adherence and acceptance of longterm therapy) • Limited use in renal dysfunction • Limited fully functional reversal agents • Decrease of AT alter efficacy of LMWH 1. Villa E et al., Enoxaparin prevents portal vein thrombosis and liver decompensation in patients with advanced cirrhosis. Gastroenterology 2012;143:1253-1260. 2. Amitrano L et al., Safety and efficacy of anticoagulation therapy with low molecular weight heparin for portal vein thrombosis in patients with liver cirrhosis. J Clin Gastroenterol 2010;44:448-451.
Which anticoagulant? • DOACs have the advantage of oral dosing. • Sparse and anecdotal data about efficacy and safety in cirrhosis: • Same efficacy and bleeding risk of traditional anticoagulants; • Data about small risk of idiosyncratic hepatotoxicity (above all rivaroxaban) Randomized controlled PVT prophylaxis studies using DOACs in cirrhosis are ongoing.
In the setting of LT, highly desirable is the presence of a direct and efficacious reversal agent for anticoagulants (time frame between last dose and major surgery unpredictable). The only DOAC reversal agent approved is idaracizumab, and its successful use in the setting of LT has been recently reported (Liver transplantation, 2017). Intagliata NM et al., Reversal of direct oral anticoagulants for liver transplantation in cirrhosis: a step forward. Liver Transpl 2017;23:396-397.
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION Anticoagulation in the setting of PVT in LT candidates is recommended. Questions: Bleeding risk? Which anticoagulant? LMWH? VKA? DOACs? Timing: immediately or after variceal treatment? Ligation/betablockers
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION A common concern when patients with cirrhosis and portal hypertension are given anticoagulants is the risk of worsening variceal bleeding. If the decision of initiating anticoagulation is taken, current guidelines recommend screening for varices by endoscopy and initiation of standard primary or secondary prophylaxis of variceal bleeding before starting treatment.
A multicenter retrospective study (Hepatology, 2015) in patients with cirrhosis having an episode of upper gastrointestinal bleeding (GIB) while being anticoagulated showed that anticoagulation is not associated with an increase in 5-day treatment failure or 6-week mortality. Cerini F et al., Impact of anticoagulation on uppergastrointestinal bleeding in cirrhosis. A retrospective multicenter study. Hepatology 2015;62:575-583.
Data from 8 studies, comprising 353 patients, that assessed the effects of anticoagulant therapy (low-weight heparin or warfarin vs no therapy) in patients with cirrhosis and PVT. • Anticoagulant therapy lasted approximately 6 months; follow-up was approximately 2 years. • Evaluation of the effect of anticoagulant treatment vs no therapy on: • Recanalization of PVT • Progression of PVT • Variceal and nonvariceal bleedings
This meta-analysis shows that anticoagulants are efficacious and safe for the treatment of PVT in cirrhosis. • It suggests also a protective role on variceal bleeding, probably due to the positive effect on portal hypertension. • LIMITATIONS: • Small sample size (only 350 cirrhotic patients) • No information about site and extension of thrombi • Non-randomized controlled trials • Need of planning interventional clinical trials with larger sample size to confirm data
MANAGEMENT OF PORTAL VEINTHROMBOSIS IN CANDIDATES FORLIVER TRANSPLANTATION Anticoagulation in the setting of PVT in LT candidates is recommended. Questions: Bleeding risk? Which anticoagulant? LMWH? VKA? DOACs? Timing: immediately or after variceal treatment? Ligation/beta-blockers
Nery F et al., Nonselective beta-blockers and the risk of portal vein thrombosis in patients with cirrhosis: results of a prospective longitudinal study. Aliment Pharmacol Ther 2019; 1-7.
Nery F et al., Nonselective beta-blockers and the risk of portal vein thrombosis in patients with cirrhosis: results of a prospective longitudinal study. Aliment Pharmacol Ther 2019; 1-7.
Association between PVT and exposure to NSBB, independently from effects on heart rate and portal blood flow velocity • Mechanisms are unknown • LIMITATIONS OF THE STUDY: • Small sample size • Short-term follow-up • Duration of NSBB not recorded • More studies are needed to understand this association and optimise targeting of nonselective beta-blockers in patients with cirrhosis Nery F et al., Nonselective beta-blockers and the risk of portal vein thrombosis in patients with cirrhosis: results of a prospective longitudinal study. Aliment Pharmacol Ther 2019; 1-7.
TAKE-HOME MESSAGES • Treatment of PVT is mandatory in the setting of LT, in order to avoid progression of thrombosis (that could cause even delisting) and allow a conventional end-to-end portal anastomotic technique, associated with a better post-LT outcome. • Anticoagulation should be started immediately, in association with an adequate prophylaxis for gastrointestinal bleeding (and maintained until liver transplantation to prevent re-thrombosis). • TIPS is another feasible option, but only in specialized centers.
TAKE-HOME MESSAGES • If the decision of initiating anticoagulation is taken, it is wise to recommend screening for varices by endoscopy and if present, adequate prophylaxis must be used. • In presence of varices, recent data suggest a possible “protective role” of anticoagulation on the risk of variceal bleeding, that has to be confirmed by further studies.