Download
1 / 34
440 likes | 1.28k Vues
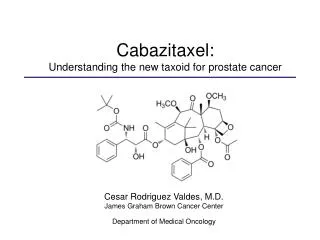
Cabazitaxel: Understanding the new taxoid for prostate cancer. Cesar Rodriguez Valdes, M.D. James Graham Brown Cancer Center Department of Medical Oncology. Learning objectives. Brief overview of prostate cancer and the mechanism of action of taxanes.

E N D
Cabazitaxel: Understanding the new taxoid for prostate cancer Cesar Rodriguez Valdes, M.D. James Graham Brown Cancer Center Department of Medical Oncology
Learning objectives • Brief overview of prostate cancer and the mechanism of action of taxanes. • Discuss the molecular properties of cabazitaxel. • Integrating concepts for second line therapy in castrate resistant prostate cancer. • Overview of advances in other study treatments.
Prostate cancer • Prostate cells store large amounts of zinc. • Produce citrate for semen. • Requires large amounts of ATP. • Cancer cells do not accumulate zinc. • Lack ZIPI transporter. • Use stored energy for cell division. • Second most common malignant tumor in men. • 25% of new cancer diagnoses.
Prostate cancer management • Important distinction in staging: prostate confinement. • Local and regional stages have a 100% 5-year survival. • Treatment for localized disease: • Surveilance (stage I) • Surgical resection or cryosurgery • Radiation therapy • Brachytherapy • External beam radiation • High intensity focused ultrasound (HIFU)
Prostate cancer management • Metastatic disease is not curable. • Treatment achieves temporary disease control. • Treatment of metastatic disease: • Hormone ablation therapy. • Orchiectomy • Gonadotropin releasing hormone agonists. • Antiandrogens. • Estrogens • Chemotherapy Most become Refractory after 1-3 years.
Overview of taxanes • Hydrocarbons (diterpenes) originating from pinetrees, butterflies or termites. • Disrupt microtubule function. • Stabilization against cold-induced. depolimerization. • Radiosensitizing
Microtubule dynamics Hydrolysis and growth Dissociation and rescue Tubulin GTP- bound GDP- bound
Molecular structure cabazitaxel docetaxel
Advantages of cavezitaxel • Semi-synthetic taxane. • Cavazitaxel is more cytotoxic towards MDR1- expressing tumor cells. What is the MDR1 gene (ABCB1)? • Encodes an ATP-dependent P-glycoprotein. • Membrane protein that works as a drug efflux pump. • Has broad substrate specificity. • Responsible for decreased drug accumulation in multidrug-resistant cells. • Functions as a transporter in the blood-brain barrier.
Vol 15 Oct 7,2004
TAX 327 trial • Study type: randomized non-blinded Phase III multicenter trial. • 24 countries • Population: 1006 patients with metastatic CRPC. Study Objectives: • Primary goal: overall survival. • Secondary: pain control, PSA levels, quality of life.
docetaxel q3 weeks - 75 mg/m2 every 3 weeks - prednisone 5mg PO twice daily mitoxantrone - 12 mg/m2 every 3 weeks - prednisone 5mg PO twice daily docetaxel weekly - 30 mg/m2 weekly - prednisone 5mg PO twice daily TAX 327 trial (cont’d) 1006 patients Metastatic CRPC on • Inclusion criteria • - confirmed diagnosis of metastates • progression of dz while on hormone treatment • Karnofsky of at least 60 • no cytotoxic pretreatments • 4 weeks of being off antiandrogens
Cabazitaxel or mitoxantrone with prednisone in patients with metastatic castration-resistant prostate cancer previously treated with docetaxel: Final results of a multinational phase III trial. TROPIC trial A.O. Sartor, S. Oudard, el al.
TROPIC trial • Phase III clinical trial
TROPIC study design Cabazitaxel 25mg/m2 q 3 wk + oral prednisone 10 mg daily for 10 cycles N=378
TROPIC trial (cont’d) • Pre-protocol treatments
TROPIC trial (cont’d) Kaplan-Meier overall survival curve Cabazitaxel + prednisone Cabazitaxel + prednisone
TROPIC trial (cont’d) • Subgroup overall survival analyses
TROPIC trial (cont’d) • Secondary endpoint: progression free survivial
TROPIC trial (cont’d) • Secondary endpoint: response and time to progression
TROPIC trial (cont’d) • Adverse events
TROPIC trial (cont’d) • Adverse events
TROPIC trial (cont’d) • Deaths during study
TROPIC trial summary • Cabazitaxel has a statistical and clinical significant improvement in OS compared to mitoxantrone treated patients. • OS: 15.1 vs 12.7 months • 30% risk reduction of death (HR=0.7, P<0.0001) • Grade 3/4 side effects are more significant than mitoxantrone treatment. • More neutropenic fevers, diarrhea and deaths caused by treatment.
Sipuleucel-T • Patient’s antigen presenting cells (APC) co-cultured with a fusion protein of prostatic acid phosphates (PAP). • Granulocyte-macrophage colony stimulating factor. Phase III trials (D9901 and D9902A) with 225 CRPC patients. - IMPACT trial • Sipuleucel-T vs placebo • 33% reduction in risk of death (HR 1.50; 95% CI: 1.10, 2.05; p=0.011) • Median survival 23.2 months vs 18.9 months. • 72% of placebo patients who progressed received sipuleucel Higano et al.Cancer 2009
Denosumab • Human monoclonal antibody designed to target RANKL ligand. • Leads to inhibition of osteoclast maturation. • Approved for postmenopausal women at risk of osteoporosis. Phase II study on patients with metastatic bone disease. • Urinary N-telopeptide (uNTx) levels in patients treated with denosumab vs biphosphonates. • Levels normalized in 71% and 29% respectively. Phase III trial (NCT00321620) with 1,901 CRPC patients. • Denosumab vs zoledronic acid. • Skeletal-related events. Di Lorenzo et al. Drugs 2010