Download
1 / 1
30 likes | 778 Vues
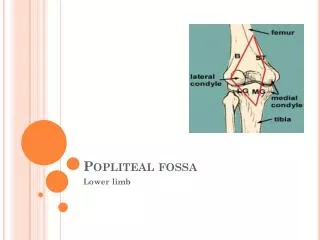
Popliteal Artery Entrapment Syndrome Allison Croucher D.O., Murtuza Habeeb M.D. Advocate Christ Medical Center Hope Children’s Hospital. Introduction:.

E N D
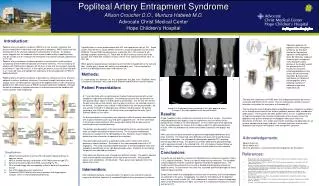
Popliteal Artery Entrapment Syndrome Allison Croucher D.O., Murtuza Habeeb M.D. Advocate Christ Medical Center Hope Children’s Hospital Introduction: Operative approach for popliteal artery entrapment syndrome. A, Standard incision for the posterior approach to the popliteal fossa. B, Operative exposure showing type I entrapment and subsequent sharp division of the medial head of the gastrocnemius. C, Successful release of undamaged popliteal artery (artery will not need to be replaced). D, Successful saphenous vein bypass of injured popliteal artery following myotomy (if indicated at operative exploration).[4] Popliteal arteryentrapment syndrome (PAES) is a rare vascular syndrome that causes claudication in adults but rarely presents in pediatrics. PAES results from the compression of the artery by adjacent musculoskeletal structures. An autopsy series suggests that the incidence of the anatomic abnormality of popliteal artery may be as high as 3.5% although the entrapment may only be clinically significant in 0.17%. [3] Popliteal artery entrapment syndrome presents in young active, healthy patients complaining of intermittent claudication of the lower extremity. The vast majority of patients with PAES present between 30-40 years of age with the youngest reported case being a 7 year old male.[1] In this report, we present a case of acute limb pain in a 17 year old male and highlight the importance of the consideration of PAES in pediatric patients. Popliteal artery entrapment syndrome is described as compression of the artery by adjacent muscle or tendinous structures. It was once thought to be quite rare but autopsy series revealed aberrant courses of the popliteal artery in 3.5% of patients. [3] More than 350 clinical cases of PAES have been published worldwide. Clinically the actual incidence of symptomatic cases is unknown because the condition still remains greatly under diagnosed. Typically there is a male predominance with M:F ratio reported as high as 15:1. Some studies estimate that in young athletic males 60% of calf claudication may be due to PAES.[6] Though PAES usually presents unilaterally, 25%-75% of patients will develop symptoms bilaterally. [1] Those with the 6th/Functional variant tend to be younger than those with anatomic variants and are more commonly female (60% vs 28%.)[6] When patients typically present complaining of intermittent claudication of the calf and foot. Initially pain is worse with activity and relieved by rest. If left untreated the patient may develop chronic lower limb ischemia [4.] Methods: In researching the literature for this presentation the key term “Popliteal Artery Entrapment Syndrome” was used in both Pubmed and MDConsult search engines. B. A. Patient Presentation: A 17 year old male with no significant past medical history presented with a chief complaint of right knee and leg pain. He stated that the pain first started when he was playing soccer about 12 months prior to presentation. For the first few months the pain occurred just with activity, now has pain at all times. He reported no pain in the left leg. Our patient was a senior in high school at the time of presentation. He was actively involved in multiple physical activities including soccer. He denied smoking or use of illicit drugs. His family history was significant for only Type II Diabetes Mellitus in his father. On first presentation to his primary care physician’s office the patient was diagnosed with a sports related muscle injury and given supportive care. He then came back to the primary care physician’s office weeks later stating that the pain was not resolving but was instead worsening. The location and description of the pain prompted the primary care physician to order an Doppler ultrasound of lower extremity. The ultrasound showed total occlusion of a segment of the right popliteal artery. Based on these findings the patient was then referred on to specialist for evaluation. The patient did not present to a specialists office until 5 months after referral because of social limitations. Evaluation at this time prompted referral for a CT angiogram. This study showed complete occlusion of the right popliteal artery and suboptimal opacification of the right dorsalis pedis artery. Based on these findings the patient was admitted for treatment. Initial admission physical exam showed no significant findings. The patient reported some mild discomfort on palpation of the right lower extremity. Dorsalis pedis pulses were recorded as +2/4 bilaterally. These pulses were palpated when the patient was at rest. The long term implications of PAES when left undiagnosed include permanent narrowing and fibrosis of the vessel. This can lead to post-stenotic aneurysm formation and makes the area prone to thrombosis[5.] The key physical exam finding to diagnose popliteal artery entrapment syndrome is the through examination of the femoral, popliteal, posterior tibial, and dorsalis pedis pulses. These pulses will often appear normal at rest. In popliteal artery entrapment syndrome the muscular compression of the vessels causes the popliteal artery pulses to decrease or disappear with plantar flexion or dorsiflexion of the foot. This simple examination technique should be done on all patients complaining of lower limb pain. A through exam can lead to earlier diagnosis and treatment of Popliteal artery entrapment syndrome. C. Image A & B demonstrating narrowing of the right popliteal artery. In Image C the right popliteal artery cannot be seen. Results: A type 2 popliteal artery entrapment was found at the time of surgery. Our patient required popliteal artery bypass using the saphenous vein and release of the gastrocnemius tendon in his initial procedure. He was taken back to the operating room the following day for release of the medial head of the right gastrocnemius muscle. After this procedure no further constriction of previous vein bypass was noted. After successful surgical correction our patient developed good blood flow to his lower extremity. He initially had some difficulties with pain control and dizziness limiting his ambulation. He subsequently developed a popliteal DVT requiring lovenox/coumadin therapy. The patient is currently working with physical therapy and is regaining strength in the affected limb. Z.O. still requires frequent follow up with vascular surgery and frequent assessment of both limbs to assess vascular flow. Acknowledgements: Special thanks to- Sonali Mehta M.D. All of the physicians, nursing and staff that helped care for this patient Conclusions: Classifications: References: • Medial head of gastroc is normal, PA is deviated medially and has an aberrant course • MHG is located laterally, no deviation of PA. Most common type-57% • Abnormal muscle bundle from MHG surrounding the PA • PA is located deeply and entrapped by a fibrous band of the popliteus muscle • Any of the above plus vein involvement • Functional PAES. Patients with normal anatomy with hypertrophic muscles. Seen in well-conditioned athletes [2] Currently the only definitive treatment for Popliteal artery entrapment syndrome Types 1-5 is surgical correction. There is no role for endovascular treatment. The standard surgical approach involves a posterior approach through the popliteal fossa. The medial head of the gastrocnemius muscle is divided and deviated to release the popliteal artery. In cases where the artery has sustained significant damage the artery requires bypass grafting. Studies have shown that angiography many be useful in patients that have developed an occlusion in the artery. Angiography may allow for thrombolysis of the popliteal artery and any runoff vessels. [6.] Until endovascular treatments improve angiography alone is not effective because it does not remove the underlying mechanism of vessel entrapment [7.] • Bergman RA, Afifi AK, Miyauchi RM. (2011, April 4) Popliteal artery entrapment. Anatomy Atlases, retrieved from www.anatomyatlasas.org • Chan CWM, Wilson JI, Myatt A, Roberts PN. Painful leg and missing pulses: a case report. Arch Dis Child 200; 83:362-363 • DeLee et al. DeLee and Drez's Orthopaedic Sports Medicine, 3rd ed. Vol 2, Chapter 23, Section L, Vascular problems-Popliteal Artery Entrapment. MD ConsultGourgiotis S, Aggelakas J, Diagnosis and surgical approach of popliteal artery entrapment syndrome: a retrospective study. Vascular Health and Risk Mangement 2008:4(I) 83-88 • Bernheim JW, Hansen J, Faries P et al. Acute lower extremity ischemia in a 7-year-old boy: An unusual case of popliteal entrapment syndrome. New England Society for Vascular Surgery 2004; 39:1340-1343. • Kurkeija K, Scagnelli T, et al. Role of angiography in popliteal artery entrapment syndrom. Diagn INterv Radiol 2009; 15:57-60 • Tercan F, Oguzkurt L, Kizilkilic O et al. Popliteal artery entrapment syndrome. Diagn Intervent Radiol 2005; 11:222-224. • Tse SML, Laxer RM, Approach to Acute Limb Pain in Childhood. Pediatr Rev 2006;27:170-179. Intervention: After failed percutaneous revascularization, the patient was referred to vascular surgery for definitive treatment of suspected Popliteal artery entrapment syndrome.