Download
1 / 9
190 likes | 1.15k Vues
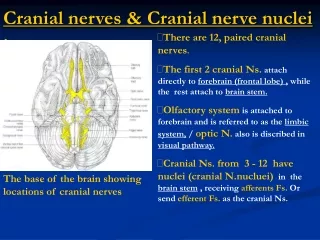
Nerve injuries . radial nerve ulnar nerve median nerves. radial nerve:. All extensors by radial n. Triceps (ex. Of elbow) , Extensor carpi radialis longus & brevis (ex. Of the wrist in radial deviation) & Brachioradialis Then divide into : Sensory:

E N D
Nerve injuries radial nerveulnarnervemedian nerves
radial nerve: All extensors by radial n. • Triceps (ex. Of elbow) , Extensor carpiradialislongus & brevis (ex. Of the wrist in radial deviation) & Brachioradialis Then divide into : Sensory: By superficial branch of radial n. which supplies Lat. 2/3 of the dorsum of the hand & the dorsal surface of the of the lat. 3 ½ fingers. Motor: By post. Interosseous n. which supplies the ex. of the forearm + supinator m. Biceps is also a supinator & it’s more stronger than supinator m.
Post. Interosseous n. injury: • weakness or paralysis of the wrist and digital extensors that’s why there’s inability to maintain finger ex. against forcible flexion. • Hand held in radial deviation when attempting wrist extension due to preservation of the radial wrist extensors but involvement of the extensor carpiulnaris and extensor digitorumcommunis. • No wrist drop. • No sensory loss. • Supination will be preserved coz there’s the biceps m.
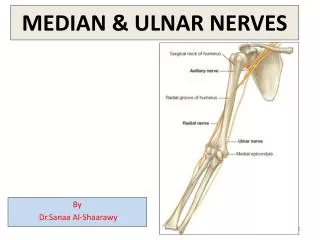
Injury to radial n. in mid arm : • Wrist drop. • Loss of sensation. • paralysis of all extensors of the wrist and digits + forearm supinators. • Only triceps is intact. Injury to radial n. high up: • Will affect triceps & every thing is gone. • It’s called Saturday night palsy. • decreased or absent sensation on the radial and dorsal side of his hand and wrist, and of inability to extend his wrist (wrist drop), thumb and finger joints.
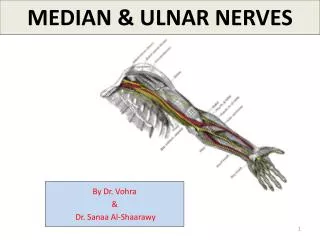
Median nerve: • The king in the forearm. Supplies 4 out of 5 :pronatorteres,flexorcarpiradialis,palmarislongus & flex. Digitorumsuperficialis. *flex. Carpi ulnaris by ulnar n. Then divide into: Sensory (the main trunk) : palmar surface of the lat. 3 ½ fingers. Motor: By ant. Interosseous n. which supplies 2 ½ out of 3 m.: Flex. Policislongus , lat. Half of flex. Digitorumprofundus & pronatorquadratus. For the hand : It gives supply to the 2 lumbricales (index & middle fingers) + all thenars m. except adductor pollicis. can be remembered using the mnemonic, "LOAF" for limbricals1 & 2, Opponenspollicis, Abductor pollicisbrevis and Flexor pollicisbrevis.
ant. Interosseous n. injury: Pts. Can't perform perfect o due to weakness of the Flexor pollicislongus muscle and the flexor digitorumprofundus at wrist level : Commonest ex. Is carpal tunnel syn. • numbness and paresthesia in the thumb, index, and middle fingers • In chronic cases, Wasting of the thenar m. • Absent abduction of the thumb. • Absent opposition of the thumb. At the level of elbow: • loss of pronation and a reduction in flexion of the hand at the wrist. • Wasting of the forearm & thenar m. • Loss of flex. Of the thumb & index fingers. Ape hand deformity : occur with an injury of the median n. either at the elbow or the wrist , impairing the thenar m. pts. Is inable to oppose the thumb and has limited abduction of the thumb.
ulnar nerve: • The king in the hand. • In the forearm: It supplies flex. Carpi ulnaris & flex. Digitorumprofundus of the little & ring fingers. In the hand: • It supplies all the interosseous m. • All the hyopthenar m. (Opponensdigitiminimi ,Abductor digitiminimi &Flexor digitiminimibrevis ). • 3rd & 4thlumbricals ( of the little & ring fingers). • One of the thenar (adductor pollicis). • & the intrinsic m. • Deep head of the Flexor PollicisBrevis. • palmarisbrevis Sensory: Dorsal & palmar aspects of the med. 1/3 of the hand & the palmar aspects of the med. 1 ½ fingers.
lesion of ulnar nerve at or near wrist : • spares the flexor carpiulnaris and the medial half of the FDP muscles • there will be loss of hypothenar muscles, interossei, adductor pollicis, third & fourth lumbricals and the deep half of the FPB. some intrinsic may continue to function due to communication between AIN and the unlnar nerve. • Froment's sign: when the patient is asked to grasp piece of paper between thumb and index finger patient will instead of doing adduction will hyperflex the IP joint to compensate for loss of the adductor pollicis • a claw-hand deformity : MCP joints are hyperextended, and the IP joints are flexed. These changes are more obvious at the ring and little fingers, because the first and second lumbrical muscles are not paralyzed. .
if ulnar nerve lesion is high up: • results in paralysis of the flexor carpiulnaris and the ulnar half of the flexor FDP muscles • clawing of ulnar two fingers without IP joint flexion because ½ of Flex. Digitorumprofundus are also paralysed. • attempt to flex the wrist results in radial deviation due to paralysis of the flexor carpiulnaris. • The patient cannot adduct or abduct the fingers +veFroment's sign.