Electrolyte Imbalance
Electrolyte Imbalance. Victor Politi, M.D., FACP, Medical Director, SVCMC, St. Anthony’s School of Allied Health Professions, PA Program. Importance of Homeostasis. Fluid and electrolyte and Acid-base balance are critical to health and well-being Maintained by intake and output

Electrolyte Imbalance
E N D
Presentation Transcript
Electrolyte Imbalance Victor Politi, M.D., FACP, Medical Director, SVCMC, St. Anthony’s School of Allied Health Professions, PA Program
Importance of Homeostasis • Fluid and electrolyte and Acid-base balance are critical to health and well-being • Maintained by intake and output • Regulation by renal and pulmonary systems
Imbalances Result From: • Illness • Altered fluid intake • Prolonged vomiting or diarrhea
Imbalances Affect: • Respiration • Metabolism Function of Central Nervous System
Distribution of Body Fluids • Water is the largest single component of the body • 60% of adult’s weight is water • Healthy people can regulate balance
Compartments • Intracellular • Within the cells • Contains dissolved solutes essential to balance • Extracellular • Outside of the cell • Interstitial • Between and around the cells • Intravascular • Also lymph and organ fluids • Within the blood vessels • Plasma
Composition of Body Fluids • Water • Electrolytes • Separates into ions when dissolved • Carries an electrical charge • Positive charge – CATIONS • Sodium, Potassium, Calcium • Negative charge – ANION • Bicarbonate, Chloride
Electrolytes • Measured in Milliequivalents per liter • mEq/L • How many grams of electrolyte (solute) in a liter of plasma (solution) • Solution is the solvent
Minerals • Constituents of all body tissues and fluids • Important in maintaining physiological processes • Act as catalysts in: • Nerve conduction • Muscle contraction • Metabolism of nutrients • Regulate electrolyte balance and hormone production • Strengthen skeletal structures IRON ZINC
Movement of Body Fluids • Cell membranes are selectively permeable • Water passes through easily • Most ions and molecules move through much slower
Osmosis • Moving a liquid through the membrane from lesser to greater solute concentration • Rate depends on concentration • Temperature • Electrical charges • Differences between osmotic pressures • Works at equalizing concentration
Osmotic Pressure (Osmolarity) • Pulling power for water • Depends on number of molecules in solution • Higher the concentration, greater pulling power • (higher osmotic pressure) • Rate is quicker • Continues until equilibrium is reached
Osmolarity • Hypertonic • Higher osmotic pressure as RBC’s • Pulls fluid from cells • Shrinks cell • Isotonic • Same osmotic pressure as RBC’s • No fluid shift • Hypotonic • Lower osmotic pressure thanRBC’s • Fluid moves into cells • Enlarges cell
Osmotic Pressure (cont) • Affected by plasma proteins • Albumin • Keeps fluid in intravascular compartment using osmotic pressure • Hydrostatic pressure draws fluid back into capillaries • Force of fluid pressure outward against surface
Diffusion • Moving a solid across the semipermeable membrane • From higher concentration to lower • To reach equilibrium • Difference between the two is concentration gradient
Filtration • Both water and solids move together in response to fluid pressure • Seen in capillary beds • ACTIVE Transport • Requires energy • Moves against gradient • Sodium and potassium pump • Uses carrier molecule • Glucose entering cell
Regulation of Body Fluids • To maintain homeostasis, fluids are regulated by: • Fluid intake • Hormonal controls • Fluid output
Fluid Intake • Regulated primarily by thirst mechanism • In the hypothalamus • Osmoreceptors monitor serum osmotic pressure • Hypothalamus stimulated when osmolarlity increases • Thirst mechanism stimulated • With decreased oral intake • Intake of hypertonic fluids • Loss of excess fluid • Stimulation of renin-angiotensisn-aldosterone mechanism • Potassium depletion • Psychological factors • Oropharyngeal dryness
Fluid Intake (cont) • Average adult intake • 2200-2700 cc/day • Oral – 1100-1400 • Solid foods – 800-1000 • Oxidative metabolism – 300 • By-product of cellular metabolism of ingested foods
Fluid Intake (cont) • Must be alert • Able to perceive mechanism • Able to respond to mechanism • **At risk for dehydration: • Elderly • Very young • Neurological disorders • Psychological disorders
Hormonal regulation • ADH • Stored in posterior pituitary gland • Released in response to changes in blood osmolarity • Makes tubules and collecting ducts more permeable to water • Water returns the systemic circulation • Dilutes the blood • Decreases urinary output
Hormonal regulation (cont) • Aldosterone • Released by adrenal cortex • In response to increased plasma potassium • Or as part of renin-angiotensin-aldosterone mechanism • Acts on distal tubules to increase reabsorption of sodium and water • Excretion of potassium and hydrogen
Hormonal regulation (cont) • Renin • Secreted by kidneys • Responds to decreased renal perfusion • Acts to produce angiotensin I • Causes vasoconstriction • Converts to Angiotensin II • Massive selective vasoconstriction • Relocates and increases the blood flow to kidney, improving renal perfusion • Stimulates release of aldosterone with low sodium
Fluid Output Regulation • Kidneys • Major regulatory organ • Receive about 180 liters of blood/day to filter • Produce 1200-1500 cc of urine • Skin • Regulated by sympathetic nervous system • Activates sweat glands • Sensible or insensible-500-600 cc/day • Directly related to stimulation of sweat glands • Respiration • Insensible • Increases with rate and depth of respirations, oxygen delivery • About 400 cc/day • Gastrointestinal tract • In stool • Average about 100-200 • GI disorders may increase or decrease it.
Regulation and Movement of Sodium • Most abundant cation in ECF • Major contributor to maintaining water balance • By effect on serum osmolality, nerve impulse transmission, regulation of acid-base balance and participation in chemical reactions • Regulated by dietary intake and aldosterone • Normal level : 135-145
Regulation and Movement of Potassium • Major cation in intracellular compartments • Regulates metabolic activities, necessary for glycogen deposits in liver and skeletal muscle, transmission and conduction of nerve impulses, normal cardiac conduction and skeletal and smooth muscle contraction • Regulated by dietary intake and renal excretion • Normal level – 3.5-5.0 • Body conserves potassium poorly • Increased urine output decreased serum potassium
Movement and Regulation of Calcium • Stored in bone, plasma and body cells (Cation) • 90% in bones • 1% in ECF • In plasma, binds with albumin • Necessary for bone and teeth formation, blood clotting, hormone secretion, cell membrane integrity, cardiac conduction, transmission of nerve impulses, and muscle contraction • Normal level – 8.5-10.5 • Regulated by bone resorption
Movement and Regulation of Magnesium • Cation • Normal 1.5-2.5 • Regulated by dietary, renal and PTH
Movement and Regulation of Chloride • Major anion in ECF • Normal level – 95-108 • Follows sodium • Regulated by dietary intake and the kidneys
Movement and Regulation of Bicarbonate • Major chemical base buffer in the body • Carbonic acid-Bicarbonate buffering system • Needed for acid-base balance • Normal level 22-26 • Regulated by kidneys
Movement and Regulation of Phosphate • Buffer anion found mainly in ICF • Assists in acid-base balance • Inversely proportional to calcium • Helps maintain healthy bones and teeth, neuromuscular activity, and CHO metabolism • Absorbed through GI tract • Normal level 2.5-4.5 • Regulated by dietary intake, renal excretion, intestinal absorption and PTH
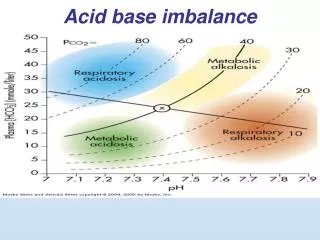
Acid-Base Balance • pH measures amount of Hydrogen ion concentration • Greater the concentration, lower the pH • 7 is neutral; <7 acidic; >7 basic or alkaline • Needed to maintain cell membrane integrity and speed of cellular enzymatic actions • Normal range – 7.35-7.45 • Regulated by buffers
Buffer • Substance or group of substances that can absorb or release hydrogen ions to correct an acid-base imbalance • Processes to regulate acid-base balance • Chemical • Biological • Physiological
Chemical Buffers (Acid-base Regulators) • Carbonic acid-bicarbonate buffer system • First to respond to changes in ECF • Acts within seconds • Increased carbon dioxide increases hydrogen ions • Carbon dioxide is excreted through lungs • Breathe faster if too high, slower if low • Hydrogen and bicarbonate ion excretion is controlled through kidneys
Biological Regulation (Buffers) • When hydrogen ions are absorbed or released by cells • Occurs in 2-4 hours • Hydrogen is positively charged, must change places with other cation, usually Potassium • With excess acid (low pH) hydrogen enters cell, potassium leaves and enters ECF • High K+ • Diabetic ketoacidosis, starvation • Chloride shift • With oxygenation of blood in the lungs, • bicarbonate diffuses into the cells; • chloride goes from hemoglobin to plasma • anion shift
Physiological Regulation (Buffer) • Lungs and Kidneys • Lungs adapt fast • Try to correct pH before biological buffers kick in • Hydrogen and carbon dioxide levels provide stimulus for respirations • Lungs alter depth and rate according to hydrogen concentration • With metabolic acidosis, respirations increase to exhale more carbon dioxide • Metabolic alkalosis, lungs retain carbon dioxide by decreasing respiraitons • Kidneys take from a few hours to several days • Reabsorb bicarbonate in case of acid excess; excrete it in cases of acid deficit
Common Disturbances Electrolyte Balance • Sodium • Hypernatremia (Na > 145, sp gravity < 1.010) • Caused by excess water loss or overall sodium excess • Excess salt intake, hypertonic solutions, excess aldosterone, diabetes insipidus, increased s water loss, water deprivation • S&S: thirst, dry, flushed skin, dry, stick tongue and mucous membranes • Hyponatremia (Na < 135, sp gravity > 1.030) • Occurs with net loss of sodium or net water excess • Kidney disease with salt wasting, adrenal insufficiency, GI losses, increased sweating, diuretics, SIADH • S&S: personality change, postural hypotension, postural dizziness, abd cramping, n&v, diarrhea, tachycardia, convulsions and coma
Common Disturbances Electrolyte Balance • Potassium • Hyperkalemia (K > 5.3; EKG irregularities-bradycardia, heart block, wide QRS pattern-cardiac arrest) • Primary cause: renal failure; major symptom: cardiac irregularity • Fluid volume deficit, massive cell damage, excess K+ given, adrenal insufficiency, acidosis, rapid infusion of stored blood, potassium-sparing diuretics • S&S: dysrhythmias, paresthesia • Hypokalemia (K < 3.5; EKG irregularities-ventricular) • Most common electrolyte imbalance; affects cardiac conduction and function. Most common cause: potassium wasting diuretics • Diarrhea, vomiting, alkalosis, excess aldosterone secretion, polyruia, extreme sweating, insulin to treat diabetic ketoacidosis • S&S: weakness, ventricular dysrhythmias, irregular pulse
Common Disturbances Electrolyte Balance • Calcium • Hypercalcemia (Ca > 5; x-rays show calcium loss, cardiac irregularities) • Frequently symptom of underlying disease with excess bond resorption and release of calcium • Hyperparathyroidism, malignant neoplastic disease, Paget’s disease, Osteoporosis, prolonged immobization, acidosis • S&S: anorexia, nausea and vomiting, weakness, kidney stones • Hypocalcemia (Ca < 4.0, EKG abnormalities) • Seen in severe illness • Rapid blood transfusion with citrate, hypoalbuminemia, hypoparathyroidism, Vitamin D deficiency, Pancreatitis, Alkalosis • S&S: numbness and tingling, hyperactive reflexes, positive Trousseau’s sign (wrist), positive Chvostek’s sign (cheek), tetany, muscle cramps, pathological fracture
Common Disturbances Electrolyte Balance • Chloride • Usually seen with acid-base imbalance • Hyperchloremia (Na >145, Bicarb <22) • Serum bicarbonate values fall or sodium rises • Hypochloremia (pH > 7.45) • Excess vomiting or N/G drainage; loop of thiazide diuretics because of sodium excretion • Leads to metabolic alkalosis due to reabsorption of bicarbonate to maintain electrical neutrality
Common Disturbances Fluid Balance • Isotonic imbalances • When water and electrolytes are gained or lost in equal proportions • Osmolar imbalances • Loss or gain of only water • Osmolality is affected
Isotonic imbalances • Fluid volume deficit (Sp Gravity > 1.025, Hct >50%, BUN > 25) • GI losses, loss of plasma or whole blood, excess perspiration, fever, decreased intake, diuretics • S&S: postural hypotension, tachycardia, dry mucous membranes, poor skin turgor, thirst, confusion, rapid weight loss, slow vein filling, lethargy, oliguria, weak pulse, sunken, dry conjunctiva • Fluid volume excess (Hct < 38%, BUN < 10 • Congestive heart failure, renal failure, cirrhosis, increased aldosterone and steroid levels, excess sodium intake • S&S: rapid weight gain, edema, hypertension, polyuria, neck vein distention, increased venous pressure, crackles in lungs
Osmolar Imbalances • Dehydration (Hyperosmolar imbalance) (Na > 145) • Diabetes insipidus, neurological damage to block thirst drive, diabetic ketoacidosis, osmotic diuresis, hypertonic IV fluids of tube feedings • S&S: dry, sticky mucous membranes, flushed and dry skin, thirst, elevated temp • Water Excess (Hypoosmolar imbalance) (Na < 135) • SIADH, excess water intake • S&S: decreased level of consciousness, convulsions, coma
Acid Base Balance • Arterial blood gas is best measure • pH • Measures hydrogen ion concentration • 7.35-7.45 • PaCO2 • Measures carbon dioxide (pulmonary ventilation) • 35-45 < hyperventilation; > hypoventilation • PaO2 • Oxygen in arterial blood • 80-100 • Oxygen Saturation • How much hemoglobin is carrying oxygen • 95-99% • Base Excess • How much blood buffer is present • High – alkalosis Caused from: Antacids, rapid blood transfusion, IV bicarb • Low – acidosis Caused from: Diarrhea • Bicarbonate • Major renal component of acid-base balance • Excreted and reproduced by kidneys • 22-26; 20 times the level of carbonic acid : low is metabolic acidosis, high alkalosis
Common Disturbances in Acid-Base Balance • Respiratory acidosis (pH <7.35; CO2> 45;) • Increased carbon dioxide, excess carbonic acid, increased hydrogen ion concentration • Causes: HYPOVENTILIATION • Atelectasis, pneumonia, cystic fibrosis, respiratory failure, airway obstruction, chest wall injury, overdose, paralysis of respiratory muscles, head injury, obesity • S&S: neurological changes and respiratory depression • Confusion, dizziness, lethargy, headache, ventricular dysrhythmias, warm flushed skin, muscular twitching
Common Disturbances in Acid-Base Balance • Respiratory alkalosis (pH > 7.45; CO2 < 35;) • Decreased carbon dioxide, decreased hydrogen ions • Causes: hyperventilation • asthma, pneumonia, inappropriate ventilator settings, anxiety, hypermetabolic state, CNS disorder, salicylate overdose • S&S: dizziness, confusion, dysrhythmia, tachypnea, numbness and tingling, convulsions, coma
Common Disturbances in Acid-Base Balance • Metabolic acidosis (pH < 7>35; Bicarb < 22) • Increased acid (hydrogen ions, decreased sodium bicarbonate • High Anion Gap (Sodium minus Chlorine + Bicarb) • Causes: starvation, diabetic ketoacidosis, renal failure, lactic acidosis, drug use (paraldehyde, aspirin) • S&S: tachypnea with deep respirations, headache, lethargy, anorexia, abdominal cramps
Common Disturbances in Acid-Base Balance • Metabolic alkalosis • Loss of acid (hydrogen ions) or increase bicarbonate • Most common cause: vomiting and gastric secretions • Hypokalemia, hypercalcemia, excess aldosterone, use of drugs (steroids, bicarb, diuretics) • S&S: numbness and tingling, tetany, muscle cramps
Variables Affecting Normal Fluid, Electrolyte and Acid-Base Imbalances • Age • Orientation status • Mobility level • Prolonged illness • Cancer, CHF, endocrine disease, COPD • Medications • Diuretics, steroids, IV therapy, TPN • Gastrointestinal losses
Clinical Assessment for Fluid, Electrolyte and Acid-Base Imbalances • History • Pre-existing disease processes • Cancer, cardiovascular, renal, GI • Age • Infants have higher % water- loss felt faster • Elderly –kidneys decreased filtration rate, less functioning nephrons, don’t excrete mediations as fast, lung changes may lead to respiratory acidosis • Acute illness • Surgery, burns, respiratory disorders, head injury • Environmental • Vigorous exercise, temperature extremes • Diet • Fluids and electrolytes gained through diet • Lifestyle • Smoking or alcohol • Medications • Side-effects may cause fluid and/or electrolyte imbalances