Download
1 / 32
380 likes | 1.37k Vues
Assessment of Abdomen. Large cavity extending from diaphragm to pelvis Vertebral column & paravertebral muscles along the back Lower rib cage & abdominal muscles in front 4 layers of large flat muscles joined midline by linea alba. Viscera.

E N D
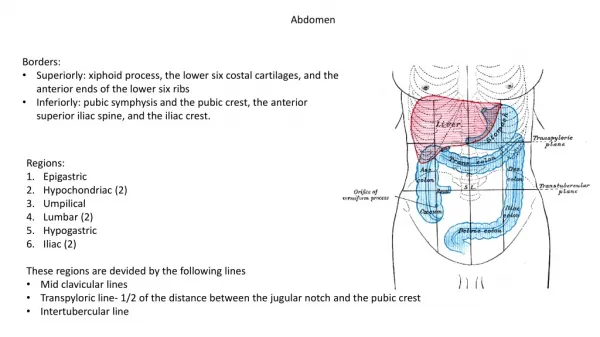
Large cavity extending from diaphragm to pelvis • Vertebral column & paravertebral muscles along the back • Lower rib cage & abdominal muscles in front • 4 layers of large flat muscles joined midline by linea alba
Viscera • VISCERA – all internal organs inside the abdominal cavity. • Solid viscera keep their shape (liver, spleen, kidneys) • Hollow viscera shape depends on contents (stomach, bladder, small intestine).
Abdominal Organs • Liver fills most of RUQ, extends over to left midclavicular line. Lower edge may normally be palpable. • Stomach lies below diaphragm between liver & spleen. • Gallbladder lies under posterior surface of liver, just lateral to midclavicular line.
Small intestine lies in all 4 quads; from stomach’s pyloric valve to RLQ where it joins the colon • Spleen lies obliquely under the diaphragm. Lymphatic tissue that runs parallel to 10th rib. Width extends from 9th to 11th rib. Not palpable normally.
Aorta lies just left of midline in upper part of abdomen, descending behind the peritoneum. 2cm below umbilicus, it bifurcates into right & left iliac arteries. • Can easily palpate aortic pulsations in upper anterior abdominal wall. • Right & left iliac arteries become femoral arteries in the groin area. Pulsations easily palpated ½ way between anterior superior iliac spine & symphysis pubis.
Pancreas is a soft lobular gland behind the stomach; lies obliquely across the posterior abdominal wall. • Kidneys are bean shaped organs that are posterior to abdominal contents; protected by posterior ribs & musculature.
Costovertebral Angle 12th rib forms an angle with the vertebral column called the costovertebral angle. Kidneys lie here at 11th & 12th ribs. Right kidney sometimes palpable b/c it lies 1-2cm lower than the left (liver on the right).
History • Appetite changes • Weight changes, over what period of time • Dysphagia • Food intolerances • Abdominal pain • N/V • Bowel history • meds
Lie anterior to pectoralis major & serratus anterior muscles between 2nd & 6th ribs; extend from side of sternum to midaxillary line. • Tail of Spence projects up & laterally into the nipple • Nipple is rough, round, & usually protrudes outward. Surface is wrinkled with milk duct openings.
Areola surrounds the nipple for 1-2cm radius. • Montgomery’s glands are small elevated sebaceous glands on the areola that secrete a protective lipid material during lactation • Areola & nipple have a darker pigmentation than the rest of the breast.
Glandular tissue • 15-20 lobes radiate from the nipple, made up of lobules. • In each lobule are clusters of alveoli that produce milk • Lobules drain into lactiferous ducts then drain milk to the lactiferous sinus (storage reservoirs behind the nipple)
Suspensory ligaments • Also called Coopers ligaments • Fibrous bands that extend vertically & attach to chest wall muscles • Give support to breast tissue
Adipose tissue • Layers of subcutaneous fat that provides the bulk of the breast • Proportion of these 3 varies depending on age, cycle, pregnancy, lactation & nutritional state.
Map out on the breast using 4 quadrants. Vertical & horizontal lines that intersect at the nipple. • UOQ contains the Tail of Spence – projects into axilla, close to pectoral group of axillary lymph nodes.
Breast Lymphatics • Central axillary lymph nodes – high up in middle of axilla • Pectoral – along the lateral edge of the pectoralis major (just inside the anterior axillary fold) • Subscapular – along the lateral edge of the scapula (deep in posterior axillary fold) • Lateral – along the humerus (inside the upper arm)
Male Breast • Rudimentary structure consisting of a thin disc of undeveloped tissue underlying the nipple • Gynecomastia- enlarged male breast tissue, usually temporary & unilateral. Occurs during adolescence & with aging • Distinguish between soft fatty enlargement of obesity and firm disc of glandular enlargement (gynecomastia)
Supernumerary Nipple During embryonic life, milk lines curve from the axilla to the groin bilaterally. The rest of the ridge usually atrophies. Occasionally a supernumerary nipple persists along the track of the mammary ridge.
Breast Self Examination • No longer ROUTINELY recommended to Canadian women. • Available evidence supports that BSE does not decrease mortality associated with breast cancer & carries the risk of potentially increasing benign biopsy rates. • BUT, if after being informed of risks & benefits of BSE, a woman makes an informed decision to perform BSE, then she should be taught to perform this self assessment screening technique proficiently
Routine Breast Health Screening • Women aged 40-69 have CBE by a trained HCP at least once every 2 years • Women aged 40-69 discuss their risk of breast cancer & the risks & benefits of routine mammography screening with their HCP • Women aged 50-69 have a screening mammogram every 2 years • Women aged 70 & older discuss routine breast cancer screening with their HCP (Canadian Cancer Society, 2008)
Canadian Statistics • 1 in 9 Canadian women will get breast cancer • If a first degree relative with breast cancer, risk is 1 in 6 • Risk of breast cancer in men is 1% or 170 cases per year • Only 5 – 10% of cancers have an identifiable breast cancer gene (BRCA1 or BRCA2) • Breast cancer is the 2nd major cause of death from cancer in women
History • Pain • Lump • Discharge • Rash • Swelling • Family hx of breast disease • Breast surgery • Self-care behaviors • Axilla tenderness, lumps, rash