Download
1 / 28
290 likes | 398 Vues
Pathophysiology of vascular tone. Arterial hypertension. Ph. D., M D. Nataliya Potikha. Regulation of arterial pressure (А P ). Formula : А P = CO · PR CO – cardiac output PR – peripheral resistance ( depended to arterioles tone ).

E N D
Pathophysiology of vascular tone. Arterial hypertension Ph. D., M D. Nataliya Potikha
Regulation of arterial pressure (АP) Formula: АP = CO · PR CO – cardiac output PR – peripheralresistance (dependedtoarterioles tone) CO leads to PR and АPnormalizes finally PR leads to COand АPnormalizes finally AP normal range: Systolic – 100-125 (equilibration 100-139) mmHg Diastolic – 70-80 (equilibration60-89) mmHg
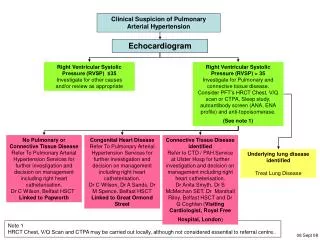
Barroreceptors of the vessels Afferent impulses Medulla oblongata (vessel’s active center) Heart (COincrease atdecreased АP) Arterioles (spasm) Еfferent і impulses Regulative systems 1. Barroreceptors of aorta arch and sinus caroticus
Regulative systems 2. Renin–angiotensinsystem Activation of kidney JGA (juxta glomerular apparatus) АP Excretion of the RENIN (it is enzyme) Conversationangiotensinogen intoangiotensin 1 Conversation angiotensin 1into angiotensin2 Angiotensin converting enzyme (АCE)
Renin Angiotensin 2 Actination of suprarenal glangs (cortical layer) Na concentration in blood increase, blood osmotic pressure increase Na reabsorbtion in kidney increase Aldosteron excretion Increase of circulative blood volume (CBV) CО increase Move of extravascular fluid inside the vessels Regulative systems 3. Renin–angiotensin-aldosteron system
Classification Arterial hypertension AP above 139/89 mm Hg Arterial hypotension Primary Secondary AP less than 100/60 mm Hg Acute Chronic
Arterial hypertension (АH) AP elevation (value above 139/89 mm Hg), which is resulted from rising of peripheral vessels resistance (one of the most common cardiovascular disorders)
Classification Primary AH (essential, hypertonic disease) Secondary AH (that is happened in 5 -10 % cases). It’s a symptom of some disease course
Etiology (primary AH) Reason is unknown. AH is polyetiological disease. AH arises on the ground of genetically peculiaritiesof metabolism. That is possible to have genetically defect of the systems, which control relaxation of the smooth muscle cells of the arterioles.
Contributing factors Age-related changes in blood pressure High salt intake Stress Family history Obesity (because hyperinsulinemia) Excess alcohol consumption (mechanism in unclear) Hyperinsulinemia: causes high activity sympathetic link of ANS and its effect on cardiac output, peripheral vascular resistance and renal sodium retention; stimulates sodium and calcium transport across the cell membrane of vascular smooth muscle, thereby sensitizing blood vessels to vasopressor stimuli Race (for example: AH isn’t only more prevalent in African Americans than whites, it is also more severe). Possible explanation: due to evolutionary adaptation to the severe environment (western Africa and Western hemisphere) in condition of salt and water deprivation survival is possible due to retention of sodium and water in organism. That leads to conserve sodium. There is little information about other racial groups
EtiologysecondaryАH • Renal • (resulted from kidney pathology) Glomerulonephritis Kidneydamage at collagenosis Uri stone disease Kidneyamiloidosis Kidneytumor Glomerulosclerosis because diabetes mellitus Nephropathy of the pregnant Hereditary defect of renal vessels Renal vessels atherosclerosis, embolism or thrombosis
EtiologysecondaryАH 2. Renoprive (arises afterkidney remove) 3. Angiogene (is caused by vessels pathology) Aorta damage Arteries carotids damage
EtiologysecondaryАH 4. Endocrinopathy (develops in the result of endocrine glands pathology) Acromegaly (Somatotropin over production by the pituitary gland anterior part) Hyperaldosteronism (aldosteronover excretion by suprarenal glands) Cushing's disease (Adrenocorticotropin over productionby the pituitary gland anterior part) Menopause (age-depended decrease of female gonads activity – estrogens excretion decrease) Possible mechanism – deficit of NO synthesis by endotheliocytes
EtiologysecondaryАH 5. Neurogene (is accompanying to nerves system pathology) Encephalitis Brain tumor Braintrauma Brainischemia Brainhemorrhage
EtiologysecondaryАH 6. Cardiac Heart defect Heart failure 7. Drug-induced Drugs, which cause vessels spasm (influent on kidney), hormonal contraceptives
Pathogenesis Increase of circulative blood volume (CBV) Emotional excitement (SNS activation) Cardiac output (CО) increase Peripheral vessels resistance increase Kidney functions violation
Pathogenesis Increase of circulative blood volume (CBV) NaCl (intakemore 5 g/day) Reasons Decrease Naexcretion by kidney (kidneydiseases)
Pathogenesis 1. CBV increase Na accumulation in vessels smooth muscle walland increase of its osmotic pressure Naretention in blood Blood osmotic pressure increase Vessels wall edema Vessels smooth musclesensitivity to vasoconstrictive influences increase (noradrenalin, adrenalin, endothelin, angiotensin) Hypervolemia Vessels narrowing Cardiac output increase Vessels spasm Peripheral vessels resistance increase AP elevation Formula: АP = CO · PR
Pathogenesis 2. Cardiac output increase (CO) Circulative blood volume increase (CBV) Reasons Emotional stress physical (overload) stress Hyperthyreosis
Pathogenesis 2. Cardiac output increase SAS activation Adrenalin excretion Increase of cardiac contractility force Increase of heart beats Increase of cardiac output AP elevation Formula: АP = CO · PR
Pathogenesis 3. SAS activation SAS activation Suprarenal glands activation Interaction adrenalin and alpha-adrenoreceptors Venues smooth muscles spasm Arterioles smooth muscles spasm Increase of circulative blood in big blood circle Noradrenalin Аdrenalin adrenoreceptors of heart alpha-adrenoreceptors of vessels Arterioles narrowing Increase of CBV PR increase Arterioles narrowing CO increase CO increase AP increase Formula: АP = CO · PR
Pathogenesis 4. Kidney functions violation Long time spasm of kidney’s arteries • Angiotensin 2 effects • Smooth muscles contraction in the vessels • Stimulation of the vasoactive center in brain • Noradrenalin excretion increase • Adrenalin excretion increase from suprarenal glands • Aldosteron excretion increase from suprarenal glands(Na retention due to kidney) AP decrease in renal capillaries Activation of JGA Renin excretion Angiotensin 2 synthesis AP increase
Depressive function of kidney – synthesis of the substances for AP reduce dilates renal arteries, reduces renin synthesis and reduces Na reabsorbing in kidney PG Е 2 ! ! ! Exhaustion of kidney depressive function leads to arterial hypertension stabilization Phospholipid Renin Inhibitor Angiotensinase Phosphatydilcholin alkali ethers
Arterial hypertension after-effects 1stperiod functional violations (heart hypertrophy) • 2dperiod • Pathological changesin arteriesand arterioles (dystrophy): • Arterioles sclerosis • Arteriole’swall infiltration by plasma (leads to dystrophy) • Arterioles necrosis (hypertonic crisis arisesin clinic) • Vein’s wall thickening
Arterial hypertension after-effects 3dperiod Secondary changes in organs and systems CNS – brain hypoxia – neurons destruction – apoplexy (because vessels destruction and rupture leads to brain hemorrhagesand brain destruction) Kidney (nephrosclerosisandchronic kidneyinsufficiency) • Organs of vision • retinopathy (retina’svessels injury) • hemorrhages and separation (exfoliation) of retina, that leads to blindness Heart Decompensate heart failure Endocrine system Glands atrophy and sclerosis