Innate Immunity-Outline
Innate Immunity-Outline. General properties Physical defenses Cellular defenses Chemical/Physiological defenses Coordinated defenses The acute phase response Inflammation Regulation of innate immunity Consequences of defects. General properties.

Innate Immunity-Outline
E N D
Presentation Transcript
Innate Immunity-Outline • General properties • Physical defenses • Cellular defenses • Chemical/Physiological defenses • Coordinated defenses • The acute phase response • Inflammation • Regulation of innate immunity • Consequences of defects
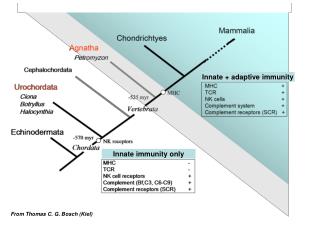
General properties • Innate immunity: 1) rapid, 2) invariant, 3) limited in specificity, and 4) the response to a particular type of microbe is not larger or faster after a previous encounter (no memory response). Innate and acquired immune components constantly interact to produce a coordinated defense system. • Contrasts with acquired immunity: 1) requires time (4 days-3 weeks) for induction, 2) variant (a unique response to each foreign substance), 3) highly specific, and 4) Second and subsequent encounters with same foreign material produces larger, more rapid response (basis for vaccination) See Parham Fig. 1.5
General Properties The innate immune system specializes. Different threats are handled by different components. For example, viruses induce interferons (IFN-a, IFN-, IFN-) which act to inhibit viral replication. Bacterial lipopolysaccharide induces chemokines and cytokines that lead to inflammation. However, there is some overlap (some common mechansims induced).
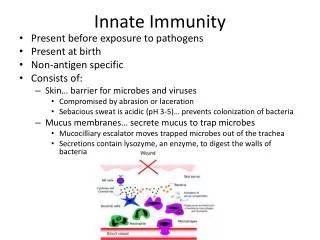
Physical barriers Fig. 1.4 • Skin, Hair, Nails • Mucosal surfaces
Other physical/chemical barriers • Mucous and ciliated cells work to trap microbes in upper respiratory tract and sweep them to the the nasal or oral cavity for expulsion or swallowing (the g.i. tract is less hospitable to microbes than the lungs) • The cough/sneeze reflex can expel large numbers of microbes (on dust or other particles) quickly • The low pH of the stomach, bile salts and acids, and digestive enzymes kill or limit growth of most microbes • Low moisture and organic acids protect skin • Competition from normal flora microbes protects from pathogens - long term antibiotic treatment can compromise this and is often associated with yeast infections because of decreased competition
Cellular defenses-Natural Killer (NK) Cells-1 • Small percentage of total lymphocytes • Kill cells infected with certain viruses • Kill susceptible cancer cells • Produce Interferon-gamma for early anti-bacterial activity • Activated by various macrophage derived cytokines (IFN-alpha, IFN-beta, IL-12) to more effectively lyse target cells Fig. 1.6c
Cellular defenses-Natural Killer (NK) Cells-2 • Recognize targets by several receptors in two families: Killer cell immunoglobulin-like receptors (KIR) and C-type lectin-like receptors (such as NKG2/CD94). These receptors recognize viral-encoded molecules, major histocompatibility molecules, or Ig Fc regions (allowing cytotoxic targeting via specific Ab) • Lysis of targets bearing self MHC I is inhibited by inhibitory receptors (mostly KIR) (cancer cells and virus infected cells often have less than normal amounts of MHC I) • Thus, targeting a cell for killing by NK cells depends on expressing a new molecule that makes it a target and decreasing expression of self MHC I Fig. 8.19
Cellular defenses-Natural Killer (NK) Cells-3 Fig. 8.20 • Receptors that recognize MHC I (HLA-A, B, or C) molecules include KIR (killer inhibitory receptor) and CD94:NKG2A
Cellular defenses-Natural Killer (NK) Cells-4 • NK cells secrete perforin (related to C9) onto the target cell surface to create a pore • Granzymes are then released, enter the target cell via a perforin pore, and induce apoptosis NK cell NK cell Target cell
Cellular defenses-Natural Killer (NK) Cells-5 • NK cells and cytotoxic T lymphocytes are complementary. NK cells kill cancer cells with low MHC class I expression and CTL kill cancer cells with high MHC I expression. Thus, the immune system may actually select for cancer cells that are resistant to the immune cell that poses the greatest threat. Fig. 12.40
Cellular Defenses-macrophages-1 Fig. 1.6 i-j • Monocytes migrate from the blood and develop into macrophages • Many tissues have resident macrophages and in some tissues they are given unique names:Kupffer cells, livermicroglial cells, CNSalveolar MØ, lungs
Cellular Defenses-macrophages-2 • Macrophages can be activated by a variety of stimuli (e.g., bacterial lipopolysaccharide, bacterial DNA, other bacterial components, phagocytosis, or T-cell derived cytokines) to produce cytokines and to prepare to kill microbes. Activation of NFkB (a nuclear transcription factor required for transcription of several cytokines) by LPS is illustrated here. Note: this figure not from Parham
Cellular Defenses-macrophages-3 • Macrophage-derived cytokines (discussed further under Inflammation are critical in coordinating innate responses to a variety of microbes. • A major effector function of macrophages is phagocytosis of particles (bacteria, yeast, etc.) or pinocytosis of viruses and the use of a variety of mechanisms to kill then and digest them. This will be discussed in greater detail in the lecture on phagocytic processes.
Cellular Defenses-Neutrophils-1 • Neutrophils are phagocytic leukocytes that are able to ingest and kill most microbes in the blood. They can migrate from blood to tissues, if needed (described more fully in the section on inflammation). • They are short lived cells and require little or no activation for maximum effect, just a triggering stimulus Fig. 1.6e
Cellular Defenses - Neutrophils-2 • Neutrophils are critically important in resistance to some microbes (e.g., gram + pyogenic cocci) and less important in resistance to other threats (e.g., cancer). • The importance of neutrophils and macrophages is probably best illustrated by the effects of defects in these cells (as in Chronic Granulomatous Disease) noted in the Immune Deficiency Foundation Web site. • Neutrophil numbers and percentage in the blood can be increased by a wide variety of conditions: extreme exercise, infection, severe psychological stress, inflammation.
Cellular Defenses - Eosinophil • Attracted to parasites (helminths or protozoa) • Secretes toxic basic proteins onto parasite surface • Can be activated by inflammatory mediators or allergens with IgE • Parasite-specific IgE greatly enhances binding to parasite • Eosinophilia is an indicator of parasitic infections Fig. 1.6f Note: this is a poor example, the granules should be more red
Cellular Defenses - Basophil • Sometimes not considered part of innate immune system because specific IgE plus antigen has been thought to be required to activate them. However, complement activation and a variety of other innate stimuli can cause activation. • Activation leads to degranulation, releasing histamine, serotonin, and eosinophil chemotactic factor
Chemical/Physiological Defenses • Lysozyme in tears and saliva kills gram + bacteria by degrading cell wall • Complement can lyse some microbes and promote their phagocytosis. It is activated by some directly • Cytokines and chemokines are important in the induction of inflammation (described in more detail later) • Interferons (IFN-a, b, and g). Induced by viruses, inhibit viral replication Figure not from Parham
Coordinated Defenses-Acute Phase Response-1 • The acute phase response is induced primarily by cytokines from macrophages, particularly IL-1, IL-6, and TNF-a whose production can be induced by the following: infection, trauma, malignant neoplasms, burns, tissue infarction, immunologically mediated inflammatory states, crystal-induced inflammatory states (gout), strenuous exercise, childbirth, and marked psychological stress. The acute phase proteins are produced mostly by hepatocytes. • The cytokines that cause the acute phase response can also act in the brain to induce fever and sleep - additional defense mechanisms.
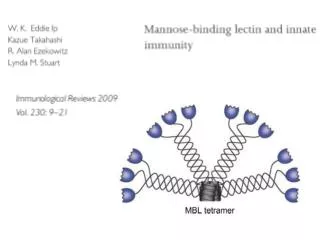
Coordinated Defenses-Acute Phase Response-2 • Acute phase proteins • Fibrinogen, blood clotting • Mannan-binding protein, opsonization • C-reactive protein, opsonization of bacteria with phosphorylcholine • Serum amyloid A protein, self-aggregation to form scar tissue - can also damage healthy organs if inappropriately deposited • SP-A and SP-D are lung surfactant proteins
Coordinated Defenses-Inflammation-1 • Characterized by four cardinal signs • Dolor (pain), calor (heat), rubor (redness), tumor (swelling) • The signs correspond to molecular and cellular mechanisms designed to bring defense mechanisms to bear on microbial invaders • Heat, caused by fever-inducing cytokines (IL-1, IL-6, TNF-a) • Redness, caused by local blood vessel dilation which is mediated by pro-inflammatory cytokines, complement, and nitric oxide • Swelling, caused by blood vessel dilation and increased vascular permeability leading to leakage of fluid from the circulation to interstitial spaces. Generally mediated by the same agents as redness • Pain, caused by stimulation of pressure sensitive nerves by swelling and release of prostaglandins (blocked by cyclooxygenase-2 (Cox-2) inhibitors)
Coordinated Defenses-Inflammation-2 • Pro-inflammatory cytokines are critical in mediating the events of inflammation. Macrophages produce all these cytokines, but some of them can be produced by other cells as well. Decreased deposition of fat, increased fatty acid oxidation Fig. 8.10
Coordinated Defenses-Inflammation-2 • Local inflammation is an essential component of host resistance to microbes • Systemic inflammation can be detrimental, even fatal. Even under normal circumstances TNF-a can contribute to cachexia and “sickness behavior” Fig. 8.12
Coordinated Defenses-Inflammation-3 • Inflammation allows cells and soluble mediators from the blood to enter sites of trauma or infection. In 1849, surgery that did not produce a robust inflammatory response (with pus, etc.) indicated a poor prognosis Fig. 1.14
Coordinated Defenses-Inflammation-4 • Inflammation can occur by strictly innate immune mechanisms. However, it can be substantially enhanced by acquired immune responses (Ab or T cell cytokines) • The characteristic pattern of cell types reflects this • Neutrophils early (first few hours) • Monocytes/macrophages later • Lymphocytes days later (if antigens are not all cleared and a specific immune response occurs)
Regulation of Innate Immunity • Regulation of cytokine responses • Activation of the HPA axis leading to increased cortisol levels and suppression of cytokine production • Upregulation of anti-inflammatory cytokines (e.g., IL-10) • Downregulation of cytokine receptors or generation of soluble (inhibitory receptors). The importance • Clearance of the microbes that induced the response
Regulation of Innate Immunity • Cellular defenses • Cortisol and clearance of microbes downregulate adhesion molecules, decreasing extravasation • If microbes cannot be cleared, response may continue with induction of additional mechanisms to isolate the microbes (e.g., tuberculosis) • Rapid apoptosis of effector cells
Consequences of innate immune deficits-1 • Effects of Innate immune defects are evident early, because these are the first line defenses. Figure not from Parham
Consequences of innate immune deficits-2 • There are a wide range of hereditary conditions that affects innate and acquired immunity. In addition to their medical relevance they inform as to the importance of particular components in immunity. You will see an example on Nov. 12. Fig. 9.7a
Consequences of innate immune deficits-3 • Several defects in leukocyte function can be suppress innate immunity Fig. 9.10
Consequences of innate immune deficits-4 • Other conditions that can adversely affect innate immunity • Compromise of barrier (burn or trauma, surgery, implanted devices that penetrate barriers) • Decreased function of ciliated cells (smoking) • Blunted cough/sneeze reflex (alcohol/drug abuse) • Immunosuppressive treatments for autoimmunity, allergy, or transplant rejection
Consequences of innate immune deficits-5 • Genetic polymorphisms may explain ethnic or individual differences in innate resistance to certain microbes (e.g., tuberculosis) • The natural resistance associated macrophage protein (Nramp1) clearly mediates differences in resistance in mouse strains, and recent studies indicate polymorphisms associated with increased susceptibility to tuberculosis in humans.