Medications and the Endocrine System
980 likes | 2.44k Vues
Medications and the Endocrine System. RN2 Medication Course School of Nursing & Health Studies Victoria University. Endocrine System. Consists of ductless glands Produce hormones that regulate and control the metabolic activities of the body, thus maintaining homeostasis

Medications and the Endocrine System
E N D
Presentation Transcript
Medications and the Endocrine System RN2 Medication Course School of Nursing & Health Studies Victoria University
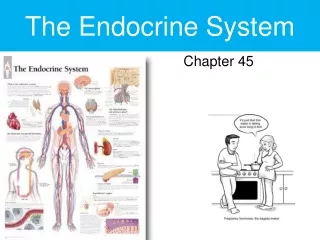
Endocrine System • Consists of ductless glands • Produce hormones that regulate and control the metabolic activities of the body, thus maintaining homeostasis • Participates in the regulation of • Digestion, use and storage of nutrients • Growth and development • Electrolyte and water metabolism • Reproductive functions
Endocrine System Overview • The nervous system coordinates rapid and precise responses to stimuli using action potentials • The endocrine system maintains homeostasis and long-term control using chemical signals (hormones) • The endocrine system works in parallel with the nervous system to control growth and maturation along with homeostasis.
Endocrine System Overview • A gland is a group of cells that produces and secretes chemicals in response to a stimulus • Exocrine glands, e.g. sweat and salivary glands, release secretions in the skin or inside the mouth via ducts (ex = outside) • Endocrine glands release more than 20 major hormones directly into the bloodstream where they can be transported to cells in other parts of the body (endo = inside)
Endocrine System Overview • Hormone enters blood & extracellular fluid • Arrives at target cell which has a protein membrane ‘receptor’. Hormone (‘key’) will only enter & ‘unlock’ a target cell ‘matched’ to that hormone; • Entry of hormone then alters the cell’s function
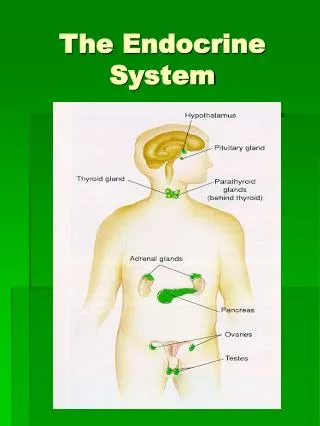
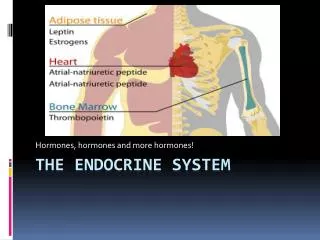
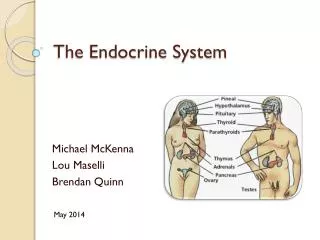
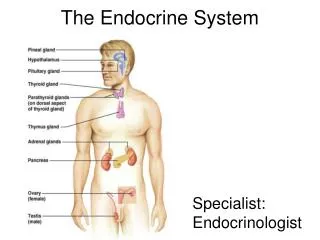
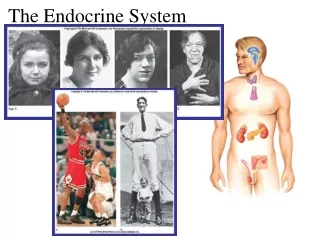
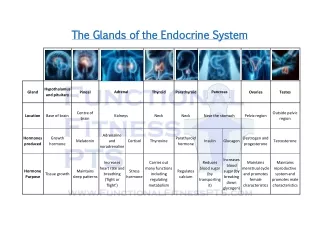
Pineal Gland Hypothalamus Pituitary Gland Anterior Posterior Thyroid Gland Parathyroid Glands Adrenal Glands Cortex Medulla Thymus Gland Pancreas Gonads Ovaries Testes Major Endocrine Glands
Endocrine control • Feedback Mechanisms • Controls and prevents the over production and underproduction of a hormone thus ensuring homeostasis • Conditions may occur due to: • A gland enlarging or shrinking in size resulting in either: • Hyper-secretion or • Hypo-secretion
Endocrine control • Hypothalamus & Pituitary. • Together they control many endocrine functions • Hypothalamus • When stimulated by feedback produces releasing factors (RF) that stimulates the pituitary to release hormones • Pituitary gland • The master gland of the body
Pituitary Gland • The hypothalamus exerts hormonal control • Pituitary gland • Size of a grape • Hangs by a stalk from the hypothalamus • Protected by the sphenoid bone • Has two functional lobes • Anterior pituitary – glandular tissue • Posterior pituitary – nervous tissue
Growth hormone • General metabolic hormone • Major effects are directed to growth of skeletal muscles and long bones • Causes amino acids to be built into proteins • Causes fats to be broken down for a source of energy
Anterior Pituitary disorders Hyperpituitarism: Increased Growth Hormone • Gigantism - during childhood or • Acromegaly - adulthood • Usually due to a slow growing adenoma • Skeletal overgrowth • Treatment • Surgery • Chemotherapy • Bromocryptine (Parlodel)
Anterior Pituitary disorders Hypopituitarism: Insufficient supply of hormones • metabolic dysfunction • sexual immaturity • growth retardation - dwarfism • Due to congennital causes, trauma, a tumour of the pituitary or hypothalamus • Replacement of hormones • Corticosteroids, thyroid & sex hormones • Growth hormone: • Somatotropin (Genotropin, Humatrope)
Posterior Pituitary Hormones • Oxytocin: stimulates contractions of the uterus & milk let-down • Antidiuretic hormone (ADH) • Can inhibit urine production • In large amounts, causes vasoconstriction leading to increased blood pressure (vasopressin)
Posterior Pituitary: Diabetes Insipidus • Deficiency of Anti Diuretic Hormone (ADH) • Causes: congenital, surgery, trauma, infection • Replacement • Vasopressin: • Pitressin: IMI/S.C/ intranasal • Desmopressin • Minirin nasal spray • Minirin, Octostim • injection IV/IMI
Thyroid Gland • Two lobes & a connecting isthmus • Controlled by hypothalamus & pituitary gland • Produces two hormones • Thyroid hormone & Calcitonin • Thyroid Hormone • Major metabolic hormone • Requires iodine • Composed of two hormones • Thyroxine (T4) – precursor • Triiodothyronine (T3) – active hormone
THYROID DISORDERS • Hyperthyroidism An over production of thyroxine causing a metabolic imbalance causing thyrotoxicosis • Hypothyroidism an underproduction of thyroxine leading to a slowing of the metabolic process causing myxoedema • Euthyroid State Normal thyroid hormone production
Tachycardia Pyrexia Hyperactivity Anxiety Moist skin Exophthalmos Possible goitre Weight loss Increased appetite Bradycardia Hypopyrexia Hypoactivity Fatigue Dry Skin Hair Loss Oedema Weight Gain Poor Memory Hyperthyroidism versus Hypothyroidism
Enlarged thyroid - GOITRE • Euthyroid – thyroid follicles/cysts • Iodine deficiency • Toxic: overproduction of thryoxin • Signs & Symptoms • neck enlargement • dysphagia • respiratory distress • Treatment depends on cause
Hyperthyroidism • Hyperthyroidism (Grave’s Disease) • Multi system autoimmune disorder characterised by pronounced hyperthyroidism, and usually associated with an enlarged thyroid gland. • Origin is unknown but may be familial. • 5 times more common in women than in men • Can arise after an infection or physical or emotional stress. • Usually occurs between 30 to 60 years of age • Treatment: • Antithyroid agents • Surgery
Exopthalmos • This is an abnormal condition marked by protrusion of the eyeballs.
Anti-Thyroid Medications • Carbimazole (Neo-Mercazole) • Decreases thyroid hormone synthesis. High dose initially then decreased to maintenance • Propylthiouracil • As above but also prevents conversion of T4 to T3 • Sodium Iodide (1311) (Radioactive) • used to reduce the production of thyroid hormones by destroying thyroid cells. • Generally used in patients who are not good surgical candidates (cardiac dysfunctions, elderly & debilitated) • Specific nursing considerations are required
Hypothyroidism • Decreased activity of the thyroid gland • Caused by: • Congenital (cretinism) • Surgical removal • Decrease of thyroid stimulating hormone (Myxoedema) • Atrophy of the thyroid gland
An auto immune thyroid disorder characterised by the production of antibodies in response to thyroid antigens. The disease shows a marked hereditary pattern. It is 20 times more common in women than in men The goitre is usually asymptomatic. Treatment: thyroxin Prognosis: good with treatment Hashimoto’s disease
Myxoedema • Signs & Symptoms • Weight gain • Mental and physical lethargy • Dryness of the skin • Constipation • Slow metabolism • Coma / death
Thyroid Medications • Thyroxine • Slow in onset but long-acting • Usually for maintenance therapy • Liothyronine (Tertroxin) • Rapidly absorbed from GIT; short-acting • Usually used for emergency therapy. • Adverse Effects • Usually decrease with time • Tremor, headache & tachycardia & Arrhythmias • GIT disturbances, weight loss
Thyroxin • Oroxine, Eutrosig • Correct storage & use essential • Unstable in light, heat, humidity • Keep in original packaging • Recommended to keep in fridge • Check expiry date • Bioavailability varies from 40-80% • Take on an empty stomach 30-60 mins pre-breakfast • Or in the evening pre bed on an empty stomach • Or with breakfast but dose will be higher & must be taken the same way each day • Decreased absorption with iron, antacids, calcium, milk, soy etc
Thyroxin • Half-life • 6-7 days Euthyroid • 3-4 days Hyperthyroid • >7 days Hypothyroid • Duration of action 7-21 days • Takes 3-4 weeks for full therapeutic effect • Levels every 6 weeks initially then 6 monthly when stable • Interactions • Increased effect - warfarin, phenobarb • Decreased effect – steroids, digoxin, hypoglycaemics
Parathyroid Glands • Tiny masses on the posterior of the thyroid • Secrete parathyroid hormone • Raise calcium levels in the blood • Stimulate osteoclasts to remove calcium from bone • Stimulate the kidneys and intestine to absorb more calcium
Calcitonin • Produced by C cells(parafollicular) in the thyroid gland • Decreases blood calcium levels by causing its deposition on bone • Antagonistic to parathyroid hormone
Parathyroid disorders • Hyperparathyroidism: an excess production of parathyroid hormone which may be due to tumours, hereditary factors or secondary to renal disease. • Causes bone decalcification and renal calculi due to an hypercalcemia • Treatment: • Calcitonin SC or IMI • Surgery
Parathyroid disorders • Hypoparathyroidism: leads to a hypocalcaemia causing neuromuscular excitability, cardiac irregularities, and digital paraesthesia • Acute ; IV calcium • Replacement: Calcium Supplements, Vit D
RN2 Medication Course School of Nursing & Health Services Victoria University Steroid Therapy
Objectives • State the functions of natural steroids • List the indications for steroid therapy • Outline the side effects of steroid therapy • Explain why steroid therapy must be gradually withdrawn • Discuss how side effects may be minimised with inhaled, topical and oral steroid therapy • Describe the patient education required for a client on steroid therapy
Adrenal glands • The medulla secretes • Adrenaline • epinephrine • Noradrenaline • Norepinephrine • The cortex secretes • Glucocorticoids • Mineralocorticoids • Androgens
Corticosteroids • Glucocorticoids • or corticosteroids or steroids • Metabolic, anti-inflammatory & immunosupressant effects • Mineralocorticoids(principally aldosterone) • Electrolyte & fluid balance via • Sodium & water retention • Potassium excretion • Androgens • Development of sex organs • Regulation of reproduction