Download
1 / 110
1.31k likes | 2.26k Vues
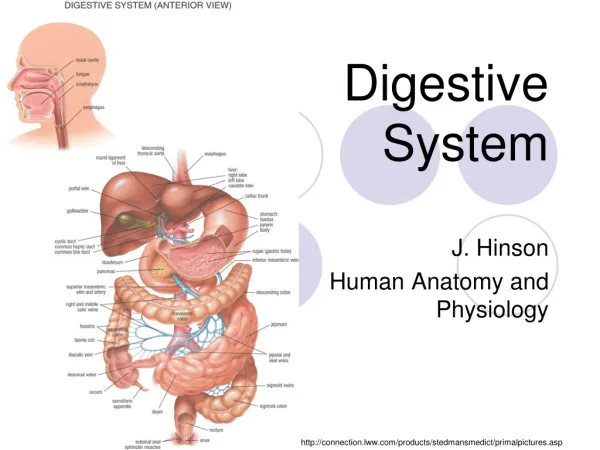
Radiology of Digestive System. Department of Radiology Zhongshan Hospital, Fudan university RAO Sheng-Xiang. Plain film radiograph. Hepatic angle Spenic angle Renal shadow Psoas muscle Properitoneal fat strip. Normal CT anatomy. 1.LHV, left hepatic vein 2.MHV, middle hepatic vein;

E N D
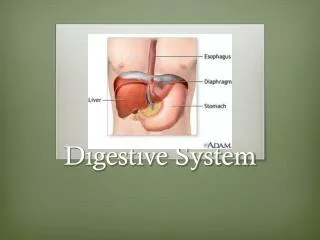
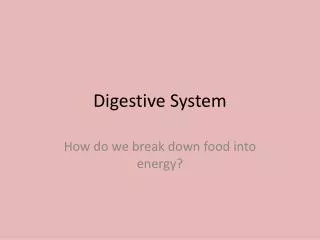
Radiology of Digestive System Department of Radiology Zhongshan Hospital, Fudan university RAO Sheng-Xiang
Plain film radiograph • Hepatic angle • Spenic angle • Renal shadow • Psoas muscle • Properitoneal fat strip
Normal CT anatomy 1.LHV, left hepatic vein 2.MHV, middle hepatic vein; 3.RHV, right hepatic vein; 4.IVC, inferior vena cava 5.Ao,aorta 6.Stomach 1 2 4 6 3 5
1.LPV, left portal vein 2.Stomach 3.Speen 4.IVC, inferior vena cava 5.Ao,aorta 1 2 4 5 3
1.Gallbladder 2.RPV, right portal vein 3.antrum 4.duodenal bulb 3 1 4 1
1.CA,celiac axis 2.Splenic artery 3.common hepatic artery 4.Duodenum 5.Kidney 6.Pancreas 7.Portal vein 8.Adrenal gland 2 6 7 3 1 4 5 5
SMA:superior mesenteric artery • CBD,common bile duct • Spenic vein • Pancreas
SMV, superior mesenteric vein • SMA, superior mesenteric artery • Uncinate process
CTA • SMA, superior mesenteric artery • CA,celiac axis • Splenic artery • common hepatic artery
main portal trunk; • right portal branch; • splenic vein; • inferior mesenteric vein; • superior mesenteric vein
RHV, right hepatic vein; • MHV, middle hepatic vein; • LHV, left hepatic vein • IVC, inferior vena cava
Upper abdominal calcification • may be an important sign of disease • Gallstones ,Porcelain gallbladder • Urinary Calculi • Calcified adrenal glands • Pancreatic calcification • Tumor calcification • ……………
Gallstones • 15% -20%of gallstones contain sufficient calcium to be identified on plain film • right upper quadrant • laminated appearance (a dense outer rim and more radiolucent center)
Porcelain gallbladder • calcification in the wall of the gallbladder • indicative of chronic obstruction of the cystic duct, chronic gallbladder inflammation, and an increased risk of gallbladder carcinoma
Discontinuous mural calcification diffuse
Kidney stones • About 85% of urinary calculi are visible on plain film. • Staghorn Calculus a large calculus occupying the collecting system of the left kidney and assuming its shape
Calcified adrenal glands • associated with adrenal hemorrhage in the newborn, tuberculosis, and Addison disease • either side of the first lumbar vertebra
Pancreatic Calcifications • chronic alcohol-induced pancreatitis • Coarse and punctate calcifications • extend upward across the left upper quadrant
Intestinal Distention • The small bowel is dilated when it exceeds 2.5 to 3.0 cm in diameter. • The colon is dilated when it exceeds 5 cm in diameter • The cecum is dilated when it exceeds 8 cm in diameter.
Normal Bowel Gas Pattern • The normal distribution of gas in the stomach and duodenum • The colon----- mottled pattern of stool • The small bowel----a few gas collections
Mechanical bowel obstruction Small Bowel • Dilated loops of small bowel (>3 cm) • Air-fluid levels that exceed 2.5 cm in length • Air-fluid levels at differing heights within the same loop (strong evidence of obstruction) • Small bubbles of gas trapped between the valvulae conniventes
Erect radiograph of the abdomen • Air-fluid levels at different heights • The valvulae conniventes that extend across the entire diameter of the bowel lumen
Mechanical bowel obstruction Large Bowel • Most colonic obstructions occur in the sigmoid colon • Dilation of the colon from the cecum to the point of obstruction • The colon distal to the obstruction is devoid of gas
Sigmoid volvulus • A large gas-filled loop(inverted U shape or a coffee bean shape) without haustra or septa, • Arising from the pelvis and extending high into the abdomen and often to the diaphragm • Barium enema: a beaking sign at the point of the twist
Adynamic ileus(Functional ileus) • Decreased or absent peristalsis • Diffuse gaseous, distension of bowel(small bowel and colon,rectum)
Pneumoperitoneum • Common causes:bowel perforation, trauma, recent surgery • Free air beneath the domes of the diaphragm
Dysphagia: Esophagus • The length of the esophagus is tubular, and its termination is saccular • A ring: the tubulovestibular junction is formed by a symmetric muscular ring • B ring : an asymmetric mucosal ring or notch that occurs at the junction of esophageal squamous epithelium with gastric columnar epithelium
The esophageal vestibule demarcated by the muscular A ring and the mucosal fold of the B ring • B ring (mucosal ring) <14mm---always symptomatic 14mm-20mm--50% symptomatic >20mm---asymptomatic
Benign Stricture Resulting from Reflux Esophagitis • usually confined to the distal esophagus • may be tapered, smooth, and circumferential (the classic appearance)
Esophageal carcinoma Four basic radiographic patterns • An annular constricting lesion, appearing as an irregular ulcerated stricture, is most common. • The polypoid pattern causes an intraluminal filling defect • The infiltrative variety grows predominantly in the submucosa and may simulate a benign stricture. • The least common pattern is that of an ulcerated mass.
Malignant Stricture • Abrupt narrowing with irregular mucosa • The prominent shoulders are characteristic of tumor
Esophageal achalasia • usually at age 30 to 50 years • Absence of peristalsis of body of esophagus • Failure of the LES to relax with swallowing • Smooth,tapered or beaklike appearance
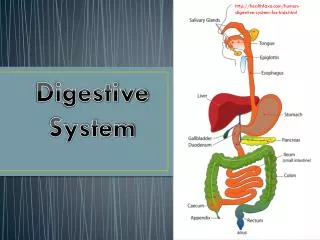
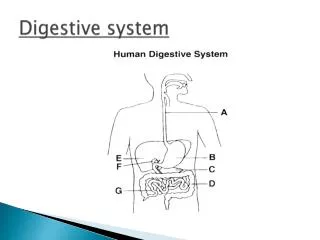
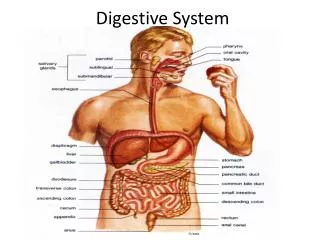
Normal anatomy of stomach • composed of the cardia, fundus, body, and antrum
A well-distended stomach has a wall thickness of approximately 5 mm
Benign Ulcer(1) • Projection beyond the lumen of stomach • soomth lucent line (collar ) at the neck of ulcer
Benign Ulcer(2) Hampton line :a thin, sharp, lucent line that traverses the orifice of the ulcer.
Benign Ulcer(3) Radiating folds extending into the crater
Malignant ulcer • location within the lumen of the stomach • nodular, rolled, irregular, or shouldered edges
Gastric adenocarcinoma • The most common malignancy in the stomach • The pattern of spread : local extension , distant metastases drop metastases to the ovaries
Polypoid Gastric Carcinoma. a lobulated filling defect (arrows) in the antrum of the stomach.
CT: • focal wall thickening • diffuse wall thickening • a lobular mass with or without ulceration • destruction of the multilayered pattern or with transmural enhancement • regional lymphadenopathy; metastases