Download
1 / 42
440 likes | 473 Vues
ALCOHOLIC LIVER DISEASE- A BRIEF INSIGHT. PRESENTED BY: VISHNU.R.NAIR, 5 TH YEAR PHARM.D, NATIONAL COLLEGE OF PHARMACY,KERALA STATE. INDEX/ CONTENTS OF THIS PPT:. GENERAL INTRODUCTION DEFINITIONS GENERAL EPIDEMIOLOGY ETIOLOGY PATHOPHYSIOLOGY OF CIRRHOSIS CLINICAL MANIFESTATIONS

E N D
ALCOHOLIC LIVER DISEASE- A BRIEF INSIGHT PRESENTED BY: VISHNU.R.NAIR, 5TH YEAR PHARM.D, NATIONAL COLLEGE OF PHARMACY,KERALA STATE.
INDEX/ CONTENTS OF THIS PPT: • GENERAL INTRODUCTION • DEFINITIONS • GENERAL EPIDEMIOLOGY • ETIOLOGY • PATHOPHYSIOLOGY OF CIRRHOSIS • CLINICAL MANIFESTATIONS • DIAGNOSIS • MANAGEMENT OF CIRRHOSIS • PATHOPHYSIOLOGY OF STEATOSIS • MANAGEMENT OF STEATOSIS
GENERAL INTRODUCTION: • ALD is defined as “LIVER DAMAGE, caused by OVER CONSUMPTION OF ALCOHOL, leading to FAT ACCUMULATION, LIVER SCARRING, and other complications. . .” • ALD mainly comprises : • ALCOHOLIC HEPATITIS(just defined in this ppt, refer other suitable areas for more details on the same) • ALCOHOLIC LIVER CIRRHOSIS(Explained more here) • ALCOLOHIC STEATOSIS(Summarized version) -NOTE: It is always advisable for readers to refer sites, books, journals and other resources for better knowledge and information nourishment. . .
DEFINITIONS: • ALCOHOLIC CIRRHOSIS: “DIFFUSE PROCESS, characterized by FIBROSIS, and CONVERSION of NORMAL HEPATIC ARCHITECTURE into STRUCTURALLY ABNORMALNODULES, owing to excess alcohol consumption. . .” 2. ALCOHOLIC STEATOSIS(FATTY LIVER): “Condition, associated with ACCUMULATION of FAT DROPLETS inside LIVERCELLS, owing to excess alcohol intake. . .” 3. ALCOHOLIC HEPATITIS: “Condition, associated with INFLAMMATION of LIVER, owing to excess alcohol intake. . .”
GENERAL EPIDEMIOLOGY: • ALD is the 3rd leading cause of death in the US • Worldwide prevalence is estimated to be around 1.7% • Worldwide mortality rate is approximately 1,50,000 deaths/ year. . .
ETIOLOGY/ CAUSES: • AGE: • High rates of morbidity observed between 45-64 years of age 2. GENDER: • Prevalence is higher in men • Susceptibility risk is higher in women 3. ETHNICITY: • CIRRHOSIS related deaths are found to be high in HISPANICS • SOUTH ASIAN MEN are more susceptible to alcohol related injury, than EUROPEANS
4. HCV INFECTION: • 14-36% of patients, with ALD, have HEPATITIS ‘C’ infection too • HCV + ALD combination increases risk for HEPATOCELLULAR CARCINOMA(HCC) reduces response to INTERFERON-ALPHA therapy 5. HBV INFECTION: • HBV + ALD combination increased risk of HCC 6. IRON OVERLOAD: • IRON + Alcohol combination generation of REACTIVE OXYGEN SPECIES Causes LIPID PEROXIDATION Leads to cell injury causes FIBROSIS, HCC, and increased risk of mortality. . .
7. MEDICATIONS: Include: • ISONIAZID • ACETAMINOPHEN • NITROFURANTOIN 8. DIET & LIFESTYLE FACTORS: Include: • Obesity • Pork products. . .
PATHOPHYSIOLOGY OF CIRRHOSIS: • Cirrhosis leads to PORTAL HHYPERTENSION(HTN), due to FIBROTICCHANGES within HEPATIC SINUSOIDS, abnormal levels of VASODILATOR & CONSTRICTOR MEDIATORS, etc. • CIRRHOSIS leads to 4 major COMPLICATIONS: • ASCITES • PORTAL HTN & ESOPHAGEAL VARICES • HEPATIC ENCEPHALOPATHY(HE) • COAGULATION/ BLEEDING DISORDERS. . .
ASCITES: • Refers to “PATHOLOGIC ACCUMULATION of LYMPH FLUID within PERITONEAL CAVITY” • Occurs, due to: • Activation of RAAS(Renin-Angiotensin-Aldosterone-System) • SODIUM & WATER retention. . . 2. PORTAL HTN & ESOPHAGEAL VARICES: - Due to PORTAL HTN VARICES(alternative routes of blood flow, from portal to systemic circulation, bypassing liver) form leads to HEMORRHAGE Causes death. ..
3. HEPATIC ENCEPHALOPATHY(HE): • Refers to “CNS DISTURBANCE, associated with wide range of NEUROPSYCHIATRIC SYMPTOMS, due to HEPATIC INSUFFICIENCY, and LIVER FAILURE(LF)” • Caused by BUILD-UP of NITROGENOUS substances in circulation • Accumulation of nitrogenous substances in circulation substances enter CNS alter neurotransmitters, that affect consciousness and behaviour • HE is of 3 types: • TYPE A: Occurs due to ACUTE LIVER FAILURE(ALF) • TYPE B: Occurs due to VARICES • TYPE C: Occurs due to CIRRHOSIS. . .
4. BLEEDING/ COAGULATION DISORDERS: • Include: • Reduced synthesis of coagulation factors • Increased fibrinolysis • Thrombocytopenia • DIC(Disseminated Intravascular Coagulation). . .
CLINICAL MANIFESTATIONS : • Hepatomegaly(Liver enlargement) • Spleenomegaly(Spleen enlargement) • Pruritus • Palmar erythema(Reddening of the palms, and occasionally, fingers) • Spider angiomata: • “Form of TELANGIECTASIS(swollen blood vessels), found slightly below the skin surface, often containing a central red spot, and reddish extensions, that radiate outwards like a spider’s web” • Also known as NEVUS ARANEUS, SPIDER NEVUS, VASCULAR SPIDER and SPIDER TELANGIECTASIS
6. Ascites 7. Pleural effusion 8. HE 9. Gynecomastia 10. Reduced libido. . .
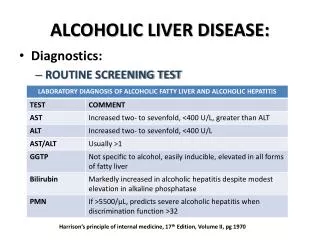
DIAGNOSIS: • Hypoalbuminemia • Raised PT • Raised ALP • Raised AST • Raised ALT • Raised GGT. . .
MANAGEMENT OF CIRRHOSIS: INCLUDES: • GOALS OF THERAPY • TREATMENT OF PORTAL HTN AND VARICES • TREATMENT OF ASCITES • SBP • TREATMENT FOR HE • NON-PHARMACOTHERAPY. . .
1. GOALS OF THERAPY: • Resolution of complications like VARICEAL BLEEDING, HE, etc • Prevention of complications • To encourage ALCOHOL ABSTINENCE • To reduce PORTAL BLOOD PRESSURE(PORTAL HTN) • To avoid morbidity and mortality • To improve HRQoL. . .
2. TREATMENT OF PORTAL HTN & VARICES: • Treatment strategies include: • PROPHYLAXIS, TO PREVENT PRIMARY BLEEDING • TREATMENT OF ACUTE VARICEAL HEMORRHAGE • PROPHYLAXIS, TO PREVENT SECONDARY BLEEDING
PROPHYLAXIS, TO PREVENT PRIMARY BLEEDING: • Usually, NON-SELECTIVE BETA-BLOCKERS are used • Drugs reduce PORTAL HTN, by: • Reducing C.O • Reducing splanchic blood flow • Usually, they need to be used for life(to prevent recurrence) • Prevent bleeding • Drugs used, include: • PROPRANOLOL( 10 mg TID) • NADOLOL (20 mg OD)
B. TREATMENT FOR ACUTE VARICEAL HEMORRHAGE: The following methods can be used: • Resuscitation • ABC(Maintain “A”irways, “B”reathing, and “C”irculation) • Sedation, as necessary • Somatostatin • Octreotide • Prophylactic antibiotics therapy • Beta-blockers • Surgical shunt • Balloon tamponade
10. Sclerotherapy 11. Terlipressin. . . NOTE: An algorithm is provided in DIPIRO text, regarding management of variceal hemorrhage. Go through the same, for a detailed understanding of this sub-division. • VASOACTIVE DRUG THERAPY: • Reduce splanchic blood flow • Reduce portal pressure • Drugs used, include: • Somatostatin • Octreotide(i.v bolus, 50-100 mcg) • Terlipressin. . .
ANTIBIOTIC THERAPY is used to prevent SEPSIS in patients, with ASCITES • EBL(Endoscopic Band Ligation) is also preferred for acute variceal bleeding) C. PROPHYLAXIS, TO PREVENT SECONDARY BLEEDING: • Usually (BETA-BLOCKERS + EBL) combination is preferred to reduce HEPATIC VENOUS PRESSURE • Drugs used include: • NADOLOL: 20-40 mg OD • PROPRANOLOL: 20 mg TID - If beta-blocker alone is not effective use the same in combination with ISOSORBIDE DINITRATE, to reduce portal pressure. . .
3. TREATMENT OF ASCITES: • Alcohol abstinence • Sodium restriction(2 g/day) • DIURETICS: • Spironolactone: 100 mg, at morning • Furosemide: 40 mg • Avoid diuretics in: • Renal insufficiency • Encephalopathy • Hyponatremia
Weight loss consideration • For tense ascites opt for PARACENTESIS(4-6L) before going for diuretics/ sodium restriction • For REFRACTORY ASCITES LIVER TRANSPLANTATION is the only option left. . .
4. SBP: • ANTIBIOTIC THERAPY is initiated to prevent SBP(Spontaneous Bacterial Peritonitis), in patients, with VARICEAL HEMORRHAGE/ ASCITES • Organisms that can cause SBP: • E. Coli • K. Pneumoniae • S. Pneumoniae • Drugs used include: • CEFOTAXIME(2 g, Q8H) • OFLOXACIN(400 mg, Q12H). . .
5. TREATMENT FOR HE: • Goals of management include: • To reverse encephalopathy • To prevent recurrence of the same • To focus on HOSPITAL/ I.P THERAPY for ACUTE HE • To focus on HOME/ O.P THERAPY for CHRONIC HE • To focus on dietary restrictions • To prevent morbidity and mortality. . .
Based on the etiological factor, therapy for HE is appropriately initiated • The following are the causes, and the therapy involved for the same: • GI BLEEDING: Treatment includes: • BAND LIGATION • SCLEROTHERAPY B. VARICEAL BLEEDING: Treatment includes: i. OCTREOTIDE
C. NON-VARICEAL BLEEDING: Treatment includes: • Endoscopic therapy • PPIs D. INFECTION/SEPSIS: Treatment includes: • ANTIBIOTICS(Depending on organism) E. ELECTROLYTE ABNORMALITIES: Treatment includes: • Discontinue DIURETICS • Fluid and electrolyte replacement
6. SEDATIVE INGESTION: Treatment involves: • Discontinue SEDATIVES/ TRANQUILIZERS • ANTIDOTE THERAPY(NALOXONE/ FLUMAZENIL) 7. DIETARY CAUSES: Treatment includes: • Limit daily protein intake(10-20 g/day) • LACTULOSE(45 ml every hour)
H. CONSTIPATION: Treatment involves: • Cathartics • Enemas • RENAL DYSFUNCTION: Treatment involves: • Discontinue DIURETICS • Discontinue NSAIDs, NEPHROTOXIC DRUGS(If patient is using) • Fluid resuscitation
Other therapies include: • METRONIDAZOLE(Those who don’t respond to diet and lactulose) • NEOMYCIN(Those who don’t respond to diet and lactulose) • ZINC ACETATE(220 mg BD) • L-ORNITHINE-L-ASPARTATE(For REFRACTORY HE). . .
6. NON-PHARMACOTHERAPY: Includes: • HOME REMEDIES FOR CIRRHOSIS • PATIENT COUNSELLING TIPS
A. HOME REMEDIES FOR CIRRHOSIS: Includes: • PAPAYA SEEDS: • Ayurvedic remedy • Helps in LIVER DETOXIFICATION II. GREEN TEA: • Green tea filled with ANTIOXIDANTS reduces oxidative stress alleviates cirrhosis
III. VITAMIN C : • VITAMIN C consists of ANTIOXIDANTS helps to prevent FATTY BUILD-UP • Increase intake of: • Amla juice(Indian Gooseberry) • Lemons • Oranges IV. ACCUPUNCTURE: • Reduces fatigue, due to cirrhosis • Also helps to abstain from alcohol consumption . . .
B. PATIENT COUNSELLING TIPS: • Reduce protein intake • Reduce salt intake • Focus on prioritizing vegetarian protein intake, compared to animal • Avoid constipation • Focus on moderate exercises • Quit alcohol consumption • Avoid processed and junk foods • Increase intake of SPINACH, CARROTS, and CABBAGE • NOTE: Over-consumption of CARROTS(rich in Vitamin A), can also lead to FIBROSIS. So consult with your dietician or physician regarding consumption of the same. . .
PATHOPHYSIOLOGY OF ALCOHOLIC STEATOSIS: • Increased ALCOHOL INTAKE Stimulates ADRENAL PITUITARY AXIS Increases LIPOLYSIS • CHRONIC ALCOHOL INTAKE leads to 2 consequences: • Inhibition of FATTY ACID OXIDATION in liver • Release of VLDL into blood • Above consequences, tantamount in the end, to STEATOSIS. . .
MANAGEMENT OF ALCOHOLIC STEATOSIS: • Alcohol abstinence • Consume foods rich in Vitamin ‘C’ & ‘E’ • Focus on a LOW FAT DIET • Correct OBESITY • Avoid high FRUCTOSE DIETS(Sodas, preserved foods, etc). . .
HOME REMEDIES FOR ALCOHOLIC STEATOSIS: • (APPLE CIDER VINEGAR+ HONEY) combination: • Reduces fat content in liver • Promotes weight loss 2. LEMON: • Contains VITAMIN C Antioxidant produces and promotes GLUTATHIONE ACTIVITY Aids in LIVER DETOXIFICATION 3. LICORICE ROOT(Avoid the same, or consult physician, if you are suffering from HYPERTENSION)
4. Indian gooseberry(Amla juice) 5. TURMERIC: • Contains CURCUMIN powerful antioxidant 6. PAPAYA 7. GREEN TEA: - According to a 2013 study in “INTERNATIONAL JOURNAL OF MOLECULAR MEDICINE” Green tea is highly effective in liver detoxification. . .
PATIENT COUNSELLING TIPS FOR STEATOSIS: • Avoid fructose diets • Avoid white flour • Consume FISH OILS • Consume FLAX SEEDS • Consume WALNUTS • Consume cabbage • Consume APPLES • Consume GUAVAS
9. Consume BLUEBERRIES 10. Avoid fatty and junk foods 11. Focus on regular, daily exercise for 30 minutes(mornings preferred) 12. Focus on weight loss strategies 13. Avoid ALCOHOL INTAKE 14. Control blood cholesterol levels 15. Control blood sugar levels. . .
THANK YOU!!!! @RXVICHU-ALWZ4UH!