Foreign Body in Throat
Foreign Body in Throat . Dr. Vishal Sharma. Aspirated (Airway) Foreign Body. Clinical Staging. 1. Initial phase: choking, coughing, wheezing, gagging 2. Asymptomatic phase: due to mucosal adaptation 3. Late phase: Laryngeal / Tracheal / Bronchial

Foreign Body in Throat
E N D
Presentation Transcript
Foreign Body in Throat Dr. Vishal Sharma
Clinical Staging 1. Initial phase: choking, coughing, wheezing, gagging 2. Asymptomatic phase: due to mucosal adaptation 3. Late phase: Laryngeal / Tracheal / Bronchial 4. Complication phase: pneumonia, emphysema, lung abscess, atelectasis
Late Clinical Features a. Laryngeal: partial or total airway obstruction, hoarseness, aphonia, hemoptysis b. Tracheal: airway obstruction, hemoptysis, wheezing, palpatory thud, auscultatory slap c. Bronchial: cough, ipsilateral wheezing, ipsilateral decreased breath sounds
Bypass valve & Stop valve effect Partial Obstruction Total Obstruction Wheezing Late Atelectasis
Check valve effect No Expiration No Inspiration Early Atelectasis Emphysema
Clinical Diagnosis Conscious pt: 1.Hoarseness / aphonia 2. Respiratory distress Unconscious pt: 1. No chest movement 2. No air exchange at nose / mouth. 3. Cyanosis.
Radio-lucent F.B. Right Lung collapse & Left emphysema
Management of choking in an unconscious patient 1. Patient placed in supine position 2. Open airway + mouth to mouth ventilation 3. Correct airway obstruction
Opening the airway • Head-tilt:Extension of neck by backward pressure on forehead
Opening the airway 2. Head-tilt, chin-lift:Extension of neck by backward pressure on forehead + lift pt’s chin keeping mouth open.
Opening the airway 3. Head-tilt, neck-lift: Lift pt’s neck while pushing down on forehead. Prevents falling back of tongue.
Opening the airway 4. Modified jaw-thrust:For pt with neck / spinal injuries. Push patient’s jaw forward by applying pressure at angle of mandible. Avoid head tilt.
Correcting airway obstruction • Back blows • Abdominal thrusts • Chest thrusts(for pregnancy, age < 8 yrs) All 3 raise subglottic pressure, to dislodge out FB • Open pt’s mouth • Blind finger sweeps in mouth
Back blows Place pt in lateral position, supporting pt’s chest against your knees. Use free hand to deliver five rapid blows to spinal Area b/w scapulae, to dislodge F.B.
Abdominal thrusts • Straddle supine pt at his hip. • Place your hand heel b/w pt’s umbilicus & ribcage, in midline. • Hold that hand with your other hand & apply 5 rapid, inward + upward thrusts, to dislodge FB.
Chest thrusts • Kneel beside supine pt at chest level.Place hand heel on centre of pt’s sternum. • Lock hands. Apply 5 rapid downward thrusts. • Only 2 fingers used for a small child.
Opening patient’s mouth Tongue-jaw lift technique: • Hold pt’s tongue + lower jaw b/w your thumb & fingers. • Lift pt’s tongue to move it away from pharyngeal wall.
Opening patient’s mouth Crossed-finger technique: • Cross your thumb under your index finger. • Place your thumb against pt’s lower lip & index finger against his upper teeth. • Uncross your fingers to open pt’s mouth.
Blind finger sweeps • Open pt’s mouth.Insert index finger of free hand into pt’s mouth, along pt’s cheek, till tongue base. Use it as a hook to roll out FB. • Avoid pushing FB further back. Avoid blind sweeps in a child. • Attempt to remove visible FB only.
Correcting airway obstruction in an unconscious pt 5 Back blows failure 5 Abdominal thrusts Or 5 Chest thrusts failure Open pt’s mouth + blind finger sweeps. Continue this sequence till FB is removed or pt is ready to be shifted to operation theatre.
Management of choking in a conscious pt • If patient can speak, cough, or breathe: Do not interfere. Patient to be examined by an ENT specialist as soon as possible. • If the patient cannot speak, cough, or breathe: Begin treatment for obstructed airway.
Correcting airway obstruction in a conscious pt > 1 yr old 5Back blows failure 5 Abdominal thrusts(Heimlich maneuver) Or5 Chest thrusts (for pregnancy, age < 8 yrs) Continue this sequence till FB is removed or pt becomes unconscious.
Back blows • Place pt in sitting / standing position. Support pt’s chest while bending pt at the waist. • Use your free hand to deliver 5 rapid blows to spinal area b/w two scapulae.
Heimlich Maneuver • Stand behind sitting / standing pt & pass your arms around pt’s waist. • Hold your fist against pt’s abdomen b/w umbilicus & ribcage. • Lock hands & apply 5 rapid, inward + upward thrusts to dislodge FB.
Chest thrusts Stand behind standing pt & pass your arms around pt’s chest.Hold your fist against pt’s sternum in its centre. Lock hands & apply 5 rapid, back- ward thrusts to dislodge FB.
Correcting airway obstruction in an infant 5 Back blows failure 5 Chest thrusts Continue this sequence till FB is removed or pt is ready to be shifted to operation theatre.
Back blows in an infant • Straddle infant face down, head lower than trunk, over your forearm, supported on your thigh. • Deliver five rapid back blows, with heel of other hand b/w shoulder blades.
Chest thrusts in an infant Supporting pt’s head, keep infant supine b/w your hands, with head lower than trunk. Using 2 fingers, deliver 5 rapid backward thrusts on sternum.
Surgical Management For life threatening stridor • Cricothyrotomy • Emergency Tracheostomy For foreign body removal • Direct Laryngoscopy • Rigid Bronchoscopy • Thoracotomy & Bronchotomy
Prevention of choking Adults: Cut food into small pieces Chew food slowly & thoroughly Avoid laughing / talking during eating Avoid excess alcohol with / before meals Infants & Children: Keep small objects away from children Avoid playing with food or toys in mouth
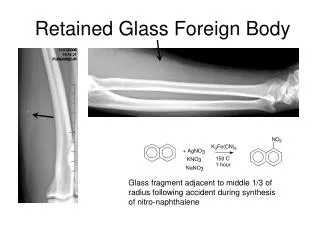
Diagnosis • Plain X-ray(PA & Lateral): soft tissue neck, chest, abdomen for radio-opaque FB • Fluoroscopy with Barium soaked cotton pledget for radiolucent FB • Barium Swallow • Flexible Oesophagoscopy
Pharyngeal FB • Common sites: tonsil, pyriform fossa, vallecula, base tongue • Diagnosis confirmed by indirect laryngoscopy • Usually removed in OPD but may require removal by Hypo-pharyngoscopy GA
Oesophageal & Gastric FB • Common sites: cricopharynx, aortic indentation & cardiac end • Usually removed by rigid oesophagoscopy GA • Advancement into stomach is safe in difficult FB • Oesophagotomy rarely required for impacted FB • FB reaching stomach, usually passes out in stool • Emetic & Cathartic agents are contraindicated
Indications for Immediate Intervention Associated respiratory obstruction Total oesophageal obstruction Disc battery (perforation occurs in 8-12 hrs) Sharp, impacted foreign body Gastro-intestinal FB > 5 cm in a child < 2 yr Gastro-intestinal FB with acute abdominal pain No progress of FB in serial X-ray after 24 hr Gastric FB with pyloric stenosis
Complications of neglected FB • Oesophageal ulceration & stricture • Oesophageal perforation mediastinitis • Peri-oesophageal cellulitis • Retro-pharyngeal abscess • Respiratory obstruction due to • tracheal compression • laryngeal oedema