FOREIGN BODY ASPIRATION
FOREIGN BODY ASPIRATION. Introduction. Children are fond of putting objects into various body orifices due to curiosity. Foreign bodies in some of the areas may be life threatening .

FOREIGN BODY ASPIRATION
E N D
Presentation Transcript
Introduction • Children are fond of putting objects into various body orifices due to curiosity. • Foreign bodies in some of the areas may be life threatening . • The lodgement of foreign bodies of all sizes,shapes and varieties in the ear and upper respiratory tract commonly affected in childhood.
Objects causing obstruction • Dry vegetable matters, seeds and nuts • Piece of carrot or popcorn • Coins, zip or buttons • Food particles like grapes, cookies, meat, apple etc.. • Latex baloon
Foreign bodies in the respiratory tract • Aspiration of foreign bodies into the respiratory tract is quite common in children. About 75% cases seeds, nuts and other vegetable matters are inhaled in airway. • Inert materials like glass beads, plastic piece, stone, screw etc can also aspirated. • Problem is common in male toddlers. • Child may present with acute airway obstruction.
Clinical features • Child with foreign body in nose- nasal obstruction, sneezing, discomfort, and sero-sanguinous discharge. • Foreign body in Larynx- Sudden choking, aphonia, stridor, violent inspiratory effort and even sudden death in case of complete obstruction. • Foreign body in Trachea- spasodic paroxysmal coughing, wheezing, hoarseness, hemoptysis, cyanosis and dyspnoea
Foreign body in bronchus- Tachypnea, cough and wheezing. Prolonged impaction may lead to pneumonitis and bronchiectasis. • Complications of long standing foreign bodies in the respiratory tract may present with repeated pneumonia, lung abscess, atelectasis, and emphysema.
Diagnosis • Clinical features • Plain chest X-Ray • Diagnostic cum therapeutic bronchoscopy
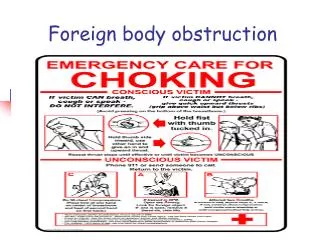
Emergency Management At Home setting- Thumping over back, groping fingers in Pharynx, Back blows, Chest thrust, Heimlich maneuver At hospital – • bronchoscopy • After bronchoscopy some children may require humidification, parenteral steroids, antibiotic and chest physiotherapy. • Tracheotomy may be required when large vegetable foreign body swells up and difficult t remove through larynx or in case of laryngeal obstruction. • Thoractotomy and bronnchotomy in case of large impacted long standing foreign body in bronchus
Foreign body in Alimentary tract • The majority ingested foreign bodies pass through stool spontaneously; some may require endoscopic or surgical removal. • Commonly ingested foreign bodies are – coins, button, cell, key, safety pin, rings, bolus of hair, cotton etc.
Clinical features: • May be similar to foreign bodies in respiratory tract but coughing is not severe and minimal choking and gagging. • Dysphagia, drooling, retrosternal / epigastric discomfort if foreign body is in esophagus. • If foreign body passes beyond esophagus it remains asymptomatic. • Impaction of foreign body in GIT may present with features of intestinal obstruction, peritonitis etc .
Diagnosis • X-Ray • Esophagoscopy • Barium studies • USG
TREATMENT • If foreign body is in esophagus- Eating bulk of mashed potatoes or banana may help • Endoscopy • Smooth surface foreign body in esophagus can be removed using Foley’s catheter. • Surgical removal • Normal diet with adequate roughage and water • Observe for untoward symptoms • Check for passage of foreign body in stool
Foreign body in eyes • Dust, sand , wood, glass etc may get embedded or enlodged into the eye • May injure cornea, conjunctiva, sclera r eye ball • Symptoms- pain, lacrimation, foreign body sensation, photophobia, redness, itching and swelling. • Severe infection may occur within hours in wood and plant foreign body
Management • Instruct to avoid rubbing • If foreign body is not embedded can remove with corner of clean cloth or blinking eyelids under clean water • Embedded foreign body – irrigation, cotton tip applicator, magnet • Surgical removal • Antibiotic therapy • Aseptic eye care • Follow up
Foreign body in ear • Pain • Discomfort • Redness • Swelling • Discharge
Measures to be taken: • Gentle suction can be used. • Ear irrigation except organic materials • insects – mineral oil or lignocain • Antibiotic ear drops • In smaller children sedation is required
Modified tweezer or forceps is used to reach and grab the object with the help of otoscope.
Foreign bodies in the nose • Most of the time asymptomatic • Pain or difficulty in breathing • Nasal bleed • Nausea/vomiting • If it gets moved towards respiratory tract • Choking, wheezing • Difficulty in breathing • Inability to talk
Management • Removal under controlled condition in a cooperative manner. • Gentle suction ( commonly used technique) • Systemic antibiotic nasal drops • Easily grasped and removed using crocodile or Tilley's forceps
Prevention • Health education to the parents • Provision of soft toys/ play materials • Do not leave minute particles at child’s vicinity • Not eating while exercising • Remind to chew food properly • Remove seeds from fruits • Do not give peanuts etc.. to the child
Reference • Hockenberry, Wilson, Judie. Wong’s essentials of pediatric Nursing. South India Edition. Elsevier publication. • Dorothy R Marlow, Barbara A Redding, Raman Kalia. Marlow’s textbook of pediatric Nursing. Harcourt Brace & Company Asia Pte Ltd. • ParulDatta. Pediatric Nursing. 4th edition. Jaypee Publishers. New Delhi.