Building Resilience in Children's Mental Health: Effective Strategies for New York's Youth
190 likes | 320 Vues
In December 2009, Dr. Mike Hogan presented key insights into children's mental health, emphasizing the urgent need for effective interventions. With 1 in 10 children facing serious emotional disturbances and alarming rates of untreated mental health issues, the need for preventive measures and early interventions has never been clearer. The Adverse Childhood Experiences (ACE) study illustrates how early trauma shapes long-term health outcomes. This presentation advocates for a comprehensive system that integrates community support and evidence-based practices to ensure every child has a chance to thrive.

Building Resilience in Children's Mental Health: Effective Strategies for New York's Youth
E N D
Presentation Transcript
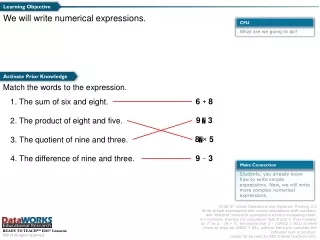
Keeping Focused in Tough Times: Building A System That Works for All New York’s Children December, 2009 Dr. Mike Hogan, OMH
Thinking Well: What We Are Called to Do • Ground our efforts in what is right, and what we know to be true. • The scope and impact of child/adolescent mental health problems • Their causes • What works, and what doesn’t
The Scope and Impact of SED: 1 out of 10 children have a serious emotional disturbance; more children suffer from psychiatric illness than from cancer, blindness, autism, mental retardation, and AIDS combined. • Only 20%+ of children with an emotional disturbance receive specialty mental health treatment. Children with mental health problems are much more likely to appear in pediatric offices and in schools than in clinics or therapist’s offices • A majority of children & youth in juvenile justice settings and with “cross-system” needs have serious emotional disturbance • Emotional disturbance is associated with the highest rate of school failure; Only 30% of children identified with emotional disturbance graduate with a standard high school diploma. • Suicide is the third leading cause of death for 15 to 24-year olds.
Developmental/Environmental Risks (Start Early in Childhood) Risks of Genetically Linked Disorders (Increase as Children enter teen years) More ER Use for Child Behavior Issues Neediest kids sent to “residential treatment”; parents give up custody to get care Depresses child’s ability to develop relationships and function independently Bipolar Disorder ADHD Depression Anxiety, depression 20% of HS Students Consider Suicide Maternal Depression: 30-50% of low income moms Chaotic parenting PTSD Conduct Disorder Many Youth in JJ /CW systems have SED Behavioral/Learning Problems Escalate Including AOD Use Learning Problems Child Abuse 50% of At Risk Students Fail to Graduate Age Birth 3 5 ELEMENTARY SCHOOL 12 MIDDLE-HIGH SCHOOL 18 To Solve Problems, Start by Understanding Them: How Children’s Behavioral Health Problems Emerge
WHY Earlier Intervention: The Adverse Childhood Experiences (ACE) Study (www.acestudy.org) • Adverse Childhood Experiences* (ACEs) are very common • ACEs are strong predictors of laterhealth risks and disease • This combination makes ACEs ‘the leading determinant of…health and social well-being’ * Psychological or physical abuse by parents; Sexual abuse; Household Dysfunction: Substance Abuse, Mental Illness, Mother Treated Violently, Imprisoned Household Member
Early Early Death Death Disease, Disability Adoption of Health-risk Behaviors Social, Emotional, & Cognitive Impairment Adverse Childhood Experiences Adverse Childhood Experiences The Influence of AdverseChildhood Experiences Throughout Life
What Works, and What Doesn’t • Targeted PREVENTIVE INTERVENTIONS are effective, underutilized • Examples: Nurse/Family Partnership, Positive Parenting Program Incredible Years, Common Sense Parenting. Include prevention • “Late Intervention” is the norm for behavioral disorders • Average age of onset for mental health problems: 14 Average lag til entering care: 9 years. Let’s intervene earlier • Early intervention with children who have experienced trauma is often very effective. Late intervention with complex trauma is often (sadly) not effective
Rates of Return from Human Capital Investment: Payoff from Investing an Extra Dollar at Different Ages (James Heckman) Rate of return to investment in human capital Programs targeted towards the earliest years Mental Health Examples to Build Resilience and Wellness: NFP, PPP, Incredible Years, Early Trauma Treatment Preschool programs Schooling Job training 0-3 4-5 Post-school School Preschool 0 Age 10/3/2014 9
What Works, and What Doesn’t • We have research-tested interventions: (e.g. MTA, TADS, MST) They share common elements that should be standard • All are multi-modal treatments, not just one thing • Parents are involved—directly or at least to support treatment • These programs are “manualized”…structured and supervised • Pay attention to specificity and “dosage.” Promote these factors • Some of the MOST EFFECTIVE tools are have are underused: • Building on strengths, not just hammering on weaknesses: resilience oriented care • The power of hope, support, welcoming • Seeing Families as Assets and Allies.Build them in, always
How To Advance The Children’s Plan In Tough Times? • Successful development of specialty children’s services: From hospital to community; Waiver and Clinic Plus • But now we see the limits of specialty services… and the major needs in all child serving sectors • The leadership and advocacy of parents and youth motivates us • Development of The Children’s Plan • The economy and budget hit the wall • Other challenges and priorities • Our approach: Roots and Wings • Sustain core capacity while we re-engineer • Grow collaborations (pediatrics, schools etc.) and learn how to grow resilience
The Threats and Opportunities We Face • The mental health buzzwords: • Recovery • Resilience • Wellness • Transformation • Our foundation (roots) are strong… and our goals (wings) are lofty. All involve change by the individuals involved, not change that is simply imposed
Clinic Reform: From Planning to Action Background: Why & How OMH Clinic Reform Briefing Oct./Nov. 2009
Why Reform? • Mental Health Clinic Services are the cornerstone of community care: • The “front door” of the specialty/public system • Used by more people than any other service; the only level of service used by most people • A critical element of care for adults with SMI and children with SED • But, there’s been no policy focus on clinic services in 20 years, while problems slowly accumulated…
Why Reform? • Problems accumulated: • Clinically: Psychiatric services undervalued, limit of one service/day, no “clinical home” concept • Fiscally: Gross inequities in reimbursement, COPS methodology unsustainable, arcane rate method used by no other payers • Legally: Billing methods not consistent with HIPAA requirements. Heavy regulation fails to achieve consistent quality. • Problems exposed: PCG Report (2007), NYS/NYS MH/CJ Report (2008)
Goals of Reform • Plan reforms collaboratively • Sustain Mental Health Clinic services as the core level of ambulatory care • Develop consistent/equitable reimbursement model that supports clinical requirements • Increase overall investment in clinics, to improve access and sustain quality • Create clinical and fiscal models that position providers better under Health Care Reform • Implement with gradual transition period allowing for adjustments, adaptation
Reform: Where We Are • Initial steps in 2008-2009 • Rate increase—lowest paid providers • Beginning of COPS reform • Elimination of “Medicaid Neutrality” provisions • “Standards of Care” posted in 2008 • Reform parameters for clinics collaboratively developed in 2008 • Reform authorized in 2009-2010 budget • Similar approach for OMH, DOH, OMRDD, OASAS licensed clinics • New “tracer” licensing approach being piloted • OMH proposed regulations filed with GORR • Implementation begins late in FY 2010 • Getting ready!
Implementation Challenges, Commitments • A better clinical model, and a better financial model for FFS Medicaid, but what about; • Medicaid MC Plans • Commercial insurers • A phased implementation plan, and how do we make “mid-course” adjustments • The essential role of leadership in change: thank you for being here and for leading