Download
1 / 53
920 likes | 1.4k Vues
Multidisciplinary approach to head and neck cancer. Kamil Konopka. Head and neck cancer (H&N). What is head & neck cancer?. Squamous cell carcinoma (90%) Mucoepidermoid carcinoma Adenoid cystic carcinoma Adenocarcinoma (lower esophagus) Small-cell carcinoma

E N D
Multidisciplinary approach to head and neck cancer Kamil Konopka
What is head & neck cancer? • Squamous cell carcinoma (90%) • Mucoepidermoid carcinoma • Adenoid cystic carcinoma • Adenocarcinoma (lower esophagus) • Small-cell carcinoma • Esthesioneuroblastoma (olfactory neuroblastoma) • Lymphomas (Hodgkin & non-Hodgkin) • Sarcomas • Melanoma • Thyroid and parathyroid cancers • Metastases
What is head & neck cancer? Majority of H&N cancers are of squamus cell origin (90%) and therefore most of clinical guidelines based on EBM apply only to squamus cell cancer. Special subtypes (sarcomas, melanomas, metastases) treatment guidelines apply both to H&N region and origin site.
Epidemiology • How can an average patient with H&N cancer be described?
Epidemiology • Account for about 3% of all cancers • M/F ratio 3:1 • Avarge age : 50 to 70 y/o. • Frequency by site: • 44% oral cavity • 31% larynx • 25% pharynx
Etiology • Tabbaco and alcohol (>75%) : effect is synergistic • UV light exposure (cancer of lips) • Diet : poor diet, especially deficient in vit.A, C, chronic iron deficiency • Genetic susceptibility: germline mutations in p53 • Other enviromental agents: formaldehyde,wood dust (adenocarcinoma of the ethmoids, nasal cavity, paranasal sinuses), radiation exposure (salivary gland tumors)
Etiology • HPV(mainly oropharyngeal cancer, less often laryngeal and oral cavity cancer) • HSV-1, HSV-2 (oral cavity) • EBV (nasopharynx, some salivary gland tumors)
Field cancerization theory • Diffuse epithelial injury throughout the head and neck, lungs and esophagus that results from chronic exposure to carcinogens. • Lifetime risk of metachronus H&N cancer is 20-40%. • Local recurences are far more often than distant metastases.
Anatomy • Complexanatomy. • Drainagepatternsissystematic and predictable.
Summary • 3% of all cancers. • 90% of squamus cell carcinoma • Male 50-70, tabacco and alcohol abuse. • HPV infeciton • Field cancerization • Complex anatomy
Multidisciplinary team • Head and neck surgery • Radiation oncology • Medical oncology • Plastic and reconstructive surgery • Specialized nursing care • Dentistry/prosthodontics • Physical medicine and rehabilitation • Spech and swallowing therapy • Clinical social work • Nutrition support • Pathology (including cytopathology) • Diagnostic radiology • Adjunctive services: • Neurosurgery • Ophtalmology • Psychiatry • Addiction services • Audiology • Palliative care
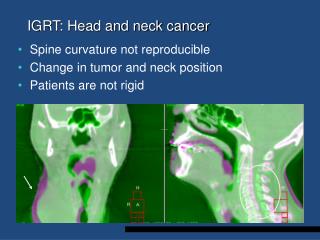
Initial assessment • Physical examination and history • Head and neck endoscopy (biopsy) • Head and neck CT-scan (or MRI, USG) • Chest X-ray, thoracic CT-scan, abdominal USG/CT • PET/CT – if high risk of distant metastases
Signs and symptoms Alterations of deglutition, phonation, hearing,respiration. • dysphagia, • odynophagia, • globus sensation, • hoarseness, • a change in the ability to form words, • epistaxis, • epiphora, • otalgia, • hemoptysis, • stuffiness of the ears, • trismus
Signs and symptoms • ORAL CAVITY: swelling or ulcer that fails to heal, ipsilateral otalgia, leukoplakia and erythroplakia • OROPHARYNX:silent area (symptoms often delayed), dysphagia, odynophagia, otalgia, neck mass • HYPOPHARYNX: silent area, dysphagia, odynophagia, otalgia, neck mass • LARYNX:persistent hoarsness, pain, otalgia, dyspnea, stridor • NASOPHARYNX: bloody nasal discharge, obstructed nostril, unilateral conductive deafness (eustachian obstruction), neurologic problems (atypical facial pain, diplopia, hoarsness, Horner’s syndrome) resulting from cranial nerve involvement, asymptomatic neck mass
Signs and symptoms • NOSE AND SINUSES: bloody nasal discharge, nasal obstruction, facial pain,facial swelling, diplopia (direct orbital extension) • PAROTID AND SUBMANDIBULAR GLANDS: local swelling +/- pain, hemifacial paralysis owing to facial nerve involvement • A METASTATIC CERVICAL NODE: may be part of the clinical presentation of any of the above-mentioned tumours
Signs and symptoms • Red flags • Any symptom that lasted for more than 2 weeks • Any asymptomatic neck mass
Diagnostic imaging • X-ray • CT • MRI • PET-CT
Biopsy • Punch or cup forceps biopsy. • FNA • Open biopsy
Pathology • Staging • Histologicgrade
Grade • G1 : >75% keratinization • G2 : 25-50% keratinization • G3 : <25% keratinization Not a consistentpredictor of clinicalbehavior. Markers of agresivebehaviour: • Perineuralspread • Lymphaticinvasion • Extracapsularextension
Staging • T score based on clinical/pathological characteristics of primary tumor • Different for every site • N/M score – similar for all sites
Staging • High impact on survival rates • Stage I >80% • Stage III/IV <40% Involvement of single lymph nodes decrease survival rate by 50%.
Principles of treatment • GOALS OF TREATMENT: a)Eradication of cancer b)Maintenance of adequate physiologic function of: -special senses (vision, hearing, balance, taste, smell) -mastication-deglutition (mandible, teeth, tongue, saliva, palate, pharynx, larynx) -respiration (larynx, trachea) -speech (larynx, tongue) c)acceptable cosmesis requires necessary but sufficient surgery, reconstructive surgical and prothesis rehabilitation MULTIDISCIPLINARY APPROACH HIGHLY RECOMMENDED
Treatmentalgorithm (oversimplified) Cancer Neoadjuvatn CTH Neoadjuvatn CTH Surgery Radical C/RTH Adjuvant RTH Adjuvant CRTH Salvagesurgery Followup
Principles of treatment: • EARLY STAGE DISEASE I, II (T1,T2,N0,M0) SINGLE MODALITY TREATMENT : SURGERY OR RADIOTHERAPY (brachytherapy) results achieved are equivalent
Principles of treatment • Decision on which modality should be choose is based onmainly on localization of tumor • Surgery : oral cavity • Radiotherapy : oropharynx, larynx, nasopharynx
Principles of treatment: ADVANTAGES OF SURGERY : -complete pathological staging of disease -quick local clearance of disease -avoidiance of toxicity of radiotherapy, including the risk of radiotherapy induced second malignancies ADVANTAGES OF RADIOTHERAPY: -avoidance of operative mortality in patients with significant comorbidities -organ conservation is more likely including preservation of the voice and swallowing -possibility of treatment of multiple synchronous primaries
Principles of treatment: • LATE STAGE DISEASE III and IV, RESECTABLE Combinedtreatment: SURGERY with adjuvant C/RTH or CHEMORADIOTHERAPY
Principles of treatment: COMBINED SURGERY + RADIOTHERAPY: 1. SURGERY + postsurgical RADIOTHERAPY -T3 – T4 primary tumour ->= N2 disease -perineural or vascular invasion -poorly differentiated tumor -short margins 2. SURGERY + postsurgical CHEMORADIOTHERAPY - positive surgical margins (cancer cells in surgical margin) - extracapsular extension
Principles of treatment: • LOCALLY ADVANCED UNRESECTABLE DISEASE –STAGE III, IV (M0) RADIOTHERAPY + CONCURRENT CHEMOTHERAPY -cisplatin most widely studied -modest survival advantage over RTH alone -increased toxicity especially mucositis
Treatmentalgorithm (oversimplified) Cancer Neoadjuvatn CTH Neoadjuvatn CTH Surgery Radical C/RTH Adjuvant RTH Adjuvant CRTH Salvagesurgery Followup
Principles of treatment: • CHEMOTHERAPY IN H&N TUMOURS: a)palliative treatment for metastatic or recurrent disease b)neoadjuvant chemotherapy c)concurrent with RTH in locally advanced H&N tumours: -improvement in locoregional control of the tumour d)Adjuvantchemotherapy (rarely) Impact on survial – 8%
Neoadjuvant chemotherapy • Performend before surgery or RTH in locally advanced disease. -reduction in distant metastases -shrinkage of tumour -organ preservation PF (cisplatin + 5FU) TPF (cisplatin + 5FU + paclitaxel) Recentstudies : negative
Biologic agent • Way to overcometoxicity of clasiccytotoxicdrugs (i.e. cisplatin) • Most widelystudied cetuximab (anty-EGFR antibody) • Used in conjunction with radiotherapy • Similaroutcomes to cisplatin, but much lowermorbidity • Less evidencethancisplatin.
H&N cancer – recurrent and metastatic disease • Goal of treatment – curative/palliative • Combinedchemotherapy (2 cytotoxics) – platin-based (cisplatin, carboplatin) • Most frequentlyusedchemotherapyregimen: cisplatin + 5-fluorouracil • Addition of cetuximab to cispl/5FU chemotherapyimprovessurvival • For patients in worsegeneralstate: monotherapy (metothrexat) • Responserate 30% and survival of 6-12 months
HPV in H&N • Emerging data areclearlyindicatingthat in a subset with positive Human PapillomaVirus (HPV) the prognosismay be betterthan for the ordinarypatient with HNSCC • Thereare data underwaywhichindicatethatHPV infectionis the most prognosticfactorwhichoutnumbersboth Tumor and Nodal status, but thisevidenceyetneeds to be betterinvestigated
HPV-associated head and neck cancer: a virus-related cancerepidemic. Lancet Oncol 2010; 11: 781–89
TAX 324 trial:induction chemotherapy TPF vs PF chemo-radiotherapy
Example • 58-year-old male patient with history of alcohol and tabacco abuse • Enlarged, palpable lymph nodes on posterior border of SCM muscle. • Palpable, ulcerated tumor in anterior 2/3 of tongue • Problems with swallowing, pain • Weight loss of 10 kg in last 4 months
Staging • CT scan of H&N : primary tumor : 3 cm • Single ipsilateral lymph nodes 2 cm. • Chest X-ray, USG : negative. • FNA : squamous cell carcinoma G2 • PS 0 • No serious comorbidites
Pretreatment : • Locoregional H&N squamous cell carcinoma • T2N1M0G2 • PS 0
Pathological report • pT3N2aG2 • Positive margins • 4 lymph nodes removed (1/4) • No additional risk factors
What now? • Second surgery (total glossectomy) • Radiochemiotherapy • Radiotherapy • Observation • ???