Enhancing Medical Education on Wards: Effective Supervision and Learning Strategies
This lecture by Dr. Deepti Rao focuses on key learning objectives for ward rotations in medical education. Attendees will learn to identify vital learning objectives, enhance daily assessments, and implement effective teaching strategies during ward rounds. The session emphasizes creating a motivating learning environment that fosters clinical diagnostic reasoning and effective supervision behaviors. Participants will engage in discussions on best practices for integrating theory and practice, using feedback, and fostering supportive interactions to optimize educational outcomes for trainees.

Enhancing Medical Education on Wards: Effective Supervision and Learning Strategies
E N D
Presentation Transcript
Teaching on the wards DeeptiRao, MD
Objectives At the end of this lecture, you should be able to: • Identify the top 5 learning objectives selected for ward rotations • Integrate various assessment and learning activities into your daily work on the wards and coordinate them with the above learning objectives • Discuss various topics including a suggestion for how ward rounds should be conducted
THE CIRCLE OF LEARNING & BERMUDA TRIANGLE OF EDUCATION Motivating Environment OBJECTIVES Pre-Existing Knowledge Meta-cognition SignificantLearning Experience ASSESSMENT CONTENT Learning with Understanding
Motivating environmentExamining what resident look for in their role models—Wright, Academic Medicine, 3/96
Motivating environmentEffective Supervisory BehaviorsEffective educational and clinical supervision, Medical Teacher 29, 2-19 • Helpful • Giving direct guidance on work • Linking theory and practice • Engaging in joint problem solving • Offering feedback • Reassurance • Ineffective • Rigidity • Low empathy • Failure to offer support • Failure to follow supervisee’s concerns • Not teaching • Being indirect and intolerant • Emphasizing evaluation and negative aspects
Motivating environmentEffective Supervisory BehaviorsEffective educational and clinical supervision, Medical Teacher 29, 2-19 • Good interpersonal skills • Involving trainees in patient care • Negotiation and assertiveness skills • Counselling skills • Appraisal skills • Self-awareness • Warmth, empathy, respect, supportive, positive, enthusiastic • Clinical competence • Teaching skills • Offering opportunities to carry out procedures • Giving direction • Giving feedback • Knowledge of teaching resources • Individualizing the teaching approach
THE CIRCLE OF LEARNING & BERMUDA TRIANGLE OF EDUCATION Motivating Environment OBJECTIVES Pre-Existing Knowledge Meta-cognition SignificantLearning Experience ASSESSMENT CONTENT Learning with Understanding
Objectives for ward rotation At the end of this ward rotation, you should be able to: • Gather data through patient history and physical to lead to a well developed problem list, differential diagnosis and management plan • Interpret technical investigations and analyze their indications • Apply clinical diagnostic reasoning skills to patient care • Demonstrate knowledge of common medical conditions • Demonstrate effective communication behaviors and skills
What are some learning activities to help us achieve these objectives • Clinical diagnostic reasoning • Observation/Checklisting • Feedback • Questions
Clinical Diagnostic Reasoning • Hypothetico-deductive (unclear diagnosis) • Scheme-inductive (dysphagia) • Pattern recognition
Educational strategies to promote clinical diagnostic reasoningJudith Bowen, NEJM 355;21
Problem representation • One sentence summary defining the specific case in abstract terms • Facilitates the retrieval of pertinent information from memory “My cough began 2 days ago. I also had a temperature of 101 and shaking. I am bringing up yellow mucus.” turns into … Acute onset of productive cough, fever, and chills in an elderly male
Semantic qualifiers • Paired, opposing descriptors that can be used to compare and contrast diagnostic considerations. • Associated with strong clinical reasoning
Illness script • Expert clinicians store and recall knowledge as simplified models (contain little knowledge about pathophys but a wealth of clinical information) that are connected to problem representations. • Conceptual models vs memories of specific syndromes or patients • Anchor points develop in the scripts based on defining and discriminating features (compare and contrast)
Educational strategies to promote clinical diagnostic reasoningJudith Bowen, NEJM 355;21
Suggestions to promote clinical diagnostic reasoning • Must see an adequate number of patients • Articulate an accurate problem representation • Different levels of learners and teacher • Reason aloud based on your problem representation and illness script/discriminating features • Compare and contrast • Force learners to prioritize differentials and explain reasoning • Students should see very typical presentations of common illnesses to solidify accurate illness scripts • Provide cognitive feedback • Reading habits • Novice learners should read about 2 related dx at same time based on a patient they have worked up
Top 9 diagnoses • Pneumonia • Poisoning and toxic effects of drugs • Cirrhosis and etoh hepatitis • Heart failure and shock • Chest pain • Gi hemorrhage • Sepsis • Disorders of pancreas • Renal failure
SNAPPS • Summarize history and findings • Narrow the differential • Analyze by comparing and contrasting • Probe the preceptor • Plan for management • Select a learning issue
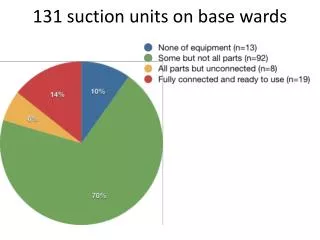
Checklisting and observation • We don’t observe our learners. • based on resident survey data summary 5/10 in answer to question, “Do faculty routinely evaluate your interview and physical exam techniques.”-26% answered no • Effectiveness of clinical rotations as a learning environment for achieving competences. Daelmans, HEM, et al, Medical Teacher, 2004 • Assuming effective learning depends on adequate supervision, feedback and assessment, a survey of medical students found that conditions for learning are poor. • “…most of the time supervision was not based on direct observation and apparently was inferred from vicarious information.”
Observation • Time • Not sure what checklists available/what are we observing for • Subject to biases • Racial and sex biases • Halo effect • Different standards
Checklisting/Observation • Mini-CEX • Structured way to give feedback • Reliable way of assessing post-grad performance • Need 12-14 observations • VA • My own experience
Feedback • We are not giving our residents feedback. • Based on Resident survey data summary 5/10 in answer to “Do all of your supervising faculty review your performance with you at the end of each rotation?” • 26% answered no
Feedback-Ende • Done with both parties working as allies • Expected and well timed • Self assessment • Based on specific actions, examples and observed behaviors • Objective
FeedbackNorcini, Workplace-based assesment as an educational tool, Medical Teacher 2007 • Encourage trainees to engage in a process of self-assessment prior to receiving external feedback • Permit trainees to respond to feedback • Ensure feedback translates into a plan of action for the trainee
Debriefing with good judgementRudolph, et al,Anesthesiology Clinics, 2007
Debriefing with good judgement • Result, action, advocacy, inquiry • “I see Mr B was not placed on antibiotics yesterday. I did not see an order for the antibiotics in powerchart. I thought we discussed placing him on antibiotics yesterday on rounds. I am wondering how you saw our discussion?”
Few tips on asking questions • Allow at least 10-15 seconds for responses • Don’t answer your own questions • Involve everyone • Open ended questions “What do you want to do?”
How do we integrate objectives, assessment and learning activities
Wards • Difficult environment • Time • Competing demands • Opportunistic learning
Residents thoughts about effective hospitalist attendings • 1. Help with scut work/seeing patients • 2. Allow the resident to run rounds however they are most comfortable • 3. Do not use residents as an information sink. Use team rounds to discuss and see higher acuity patients
Teaching attending power tips • Plan to finish by noon • Set expectations first day • Full presentations without interruption • Primary provider • Teach what you know
How should wards run • Attending and resident to meet in am and decide on acuity of patients and who is to be seen on rounds (A,B,C) • Full presentations only on sickest patients, otherwise concerning patients and discharges • If time can use to hear more about less sick/improving patients. • Attending to see less sick and stable patients on own • This allow rounds to be very efficient and can usually finish by noon
How wards should run • Make work rounds—write orders while rounding • Allow presenter to finish presentation before interrupting. At end of presentation, have presenter ask any questions they have • Allow resident or intern to answer questions first • Walk vs sit ? • Both interns vs one at a time ?
How should wards run • Maintain good working relationships with everyone from PT to consultants • Use precall days as “teaching days” by presenting articles and modules or opting to checklist notes/communication • Use the night call day to put the resident on the spot and have them formulate plans for patients. Do teaching on special topics for the resident/medical student on those days • I would propose we develop teaching activities based on each person’s area of special interest • On the post call days have other members of team formulate problem representations and problem lists for cases • Force learners to prioritize and explain differential • Observation? • Compare and contrast readings • Learning issues • Afternoons for getting work done
How should wards run? • What experience have you had with rounding and what works and what does not? • Should we be observing our learners? • How often should we give formal feedback? • How can we get our learners to self assess and use metacognition more?