Download
1 / 38
380 likes | 546 Vues
Abuse of Older Manitobans. Moira Horgan – Jones Network Coordinator. M ANITOBA N ETWORK FOR THE P REVENTION OF A BUSE OF O LDER A DULTS. Outline of Presentation. Obtain a better understanding of the prevalence of abuse of older Manitobans Differentiate types of abuse

E N D
Abuse of Older Manitobans Moira Horgan – Jones Network Coordinator MANITOBA NETWORK FOR THE PREVENTION OF ABUSE OF OLDER ADULTS
Outline of Presentation • Obtain a better understanding of the prevalence of abuse of older Manitobans • Differentiate types of abuse • Recognize risk factors • Discuss medical implications of abuse of older adults • What you should do if you suspect abuse
Introduction • Language: Elder, senior, older adult • Manitoba Network for the Prevention of Abuse of Older Adults (MNPAOA) • Mission To act as a central point of contact for provincial efforts and to support regional and community initiatives to prevent abuse of older adults. • Vision Older adults in Manitoba will live in a safe environment of respect and dignity.
Network Goals • Support Regional and Community Efforts • Develop/Adapt Education and Training Resources • Raise Public Awareness • Encourage research and advise on issues relating to abuse of older adults
Network • Funded by the Seniors and Healthy Aging Secretariat • Led by MSOS • Housed at MSOS • Over 30 partners and growing • Study of other Canadian Networks • Website • Building our Future
A Little Bit of Trivia • Classical Greek culture supported euthanasia for the incurable old. • Some ancient cultures supported ritual suicide of tribal elders during drought so food and water could be reserved for the more productive young. • King Lear – Shakespeare writes about the king’s maltreatment by his sons.
Canadian History • 1973 Newfoundland passes the Neglected Adults Welfare Act, creating a mandatory reporting obligation for “any person who has information which leads him to believe that an adult is a neglected adult...”. • Early mention of abuse & neglect in Canadian literature in the 1980s. Local service providers in some communities are beginning to identify family violence as an issue affecting older adults. • 1980 New Brunswick's Child and Family Services and Family Relations Act addresses child and adult welfare and includes disabled and older adults. • 1985 First elder abuse conference held in British Columbia (SPARC Committee on Elder Abuse) • 1986 Nova Scotia enacts the Adult Protection Act, creating a mandatory reporting duty for “every person who has information, whether or not it is confidential or privileged, indicating that an adult is in need of protection..." • 1988 Prince Edward Island enacts the Adult Protection Act. • 1989 Formation of an informal coalition in British Columbia to begin addressing abuse and neglect of older adults. Subsequently becomes the BC Coalition to Eliminate Abuse of Seniors. • 1989 The Ryerson Study, 1st national study of the prevalence of abuse and neglect in later life in Canada, is conducted. • Establishment ofthe Ontario Network for the Prevention of Elder Abuse (incorporated 1992).
Canadian History (1990) • 1990s Development of New Horizons and other Health Canada family violence prevention initiatives. These provide many Canadian communities with their first opportunity to explore abuse issues in later life. • 1990 Ontario Nursing Home Act sets out some of the rights of residents living in nursing homes. • 1991 Annual Canadian Association on Gerontology discussion meeting in Toronto: "Do We Need a Canadian Committee for the Prevention of Elder Abuse". • 1993 First national conference on elder abuse held. • 1994 B.C. Coalition to Eliminate Abuse of Seniors becomes a non profit provincial organization to raise awareness of abuse and neglect in later life. • 1998 Roundtable discussion at Canadian Association on Gerontology in Halifax, NS. "Creating a Canadian Network for the Prevention of Elder Abuse". Bylaws established and criteria developed. • 1999 2nd National Conference on Elder Abuse held in Toronto, ON. • 1998 Alberta enacts Protection for Persons in Care Act. • 1999 2nd National Conference on Elder Abuse, Toronto, Ontario, March 21-23, 1999.
Canadian History (2000) • 2000 Canadian Network for the Prevention of Elder Abuse is created as a legal entity. • 2000 British Columbia proclaims Part 3 of Adult Guardianship Act, which provides support and assistance for abused or neglected adults who are unable to seek it on their own. Encourages voluntary reporting of abuse. Recognizes community networks. • 2002 Yukon launches first Elders Conference. • 2002 Canada is the host location for the development of the Toronto Declaration on the Global Prevention of Elder Abuse. Declaration is based on the recommendations of the United Nations International Plan of Action adopted by all countries in Madrid, 2002. • 2003 Quebec Network for the Prevention of Elder Abuse is created. • 2003 Regional senior abuse prevention network develops in Alberta. • 2003 1st official recognition (proclamation) by the City of Toronto. Other cities in Ontario follow in 2003 and 2004. • 2003 1st provincial senior abuse awareness campaign (Alberta). • 2003 Yukon passes the Adult Protection and Decision Making Act, Dec. 17, 2003. Proclamation is planned for April 1, 2005. • 2004 Newfoundland and Labrador holds their first provincial conference on senior abuse. • 2004 (October 19) Ontario marks its first Elder Abuse Awareness Day.
Manitoba Achievements • 1999 Manitoba Law Reform Commission on Abuse • 2001 Manitoba proclaims Protection for Persons in Care Act. • 2002 Establishment of a Manitoba Strategy on Abuse of Older Adults • 2003 Manitoba establishes "Expect respect"initiative to help raise awareness of abuse and promote respect of older adults in the province. • 2006WEAAD June 15th • 2006 Manitoba Network for the Prevention of Abuse of Older Adults (MNPAOA) is established • 2006 Establishment of an abuse line • 2007 Establishment of a Safe Suite (A&O) • 2008 First Manitoba Conference • 2009 CAG in Winnipeg devotes one day to abuse issues • 2010 Building our Future – consultations and strategy for change
The field of prevention of abuse and neglect of older adults in Canada is lagging behind other areas of family violence prevention. It is largely the case that multiple small-scale projects and a few noteworthy larger programs exist in a patchwork of service delivery and under-coordinated effort. It is also far from being able to use practice standards such as are available for other fields (e.g. health). Promising approaches in the Prevention of Abuse and Neglect of older adults in Canada (2007) Canadian Network for the Prevention of Elder Abuse (CNPEA)
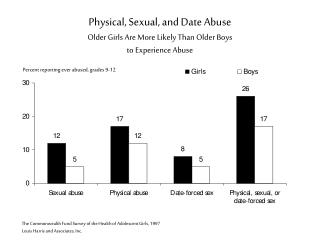
Prevalence of Elder Abuse • Actual incidence and prevalence of elder abuse is unknown and difficult to measure. • It is believed that 4 -10% of all older adults have been a victim at some time. • As part of an1999 study, 4000 older Canadians were interviewed to examine their experience regarding emotional and financial abuse as well as physical and sexual violence committed against them by children, caregivers and spouses. • approximately 7% of seniors interviewed reported that they had experienced some form of emotional or financial abuse by an adult child, caregiver or spouse within the past five years • emotional abuse was reported most frequently • financial abuse was the second most reported form of abuse • almost 2% of older Canadians reported experiencing more than one form of abuse
Why so difficult to measure? • Vast majority (80%) of cases go unreported or unsubstantiated. • Definitions of abuse od older adults can differ from agency to agency, and person to person. • Subject to cultural interpretation
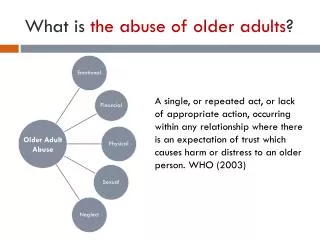
Definition of Abuse of Older Adults According to the World Health Organization, abuse and neglect of older adults can be a single or a repeated act. It can occur in any relationship where there is an expectation of trust or where a person is in a position of power or authority.
Types of Elder Abuse • Physical abuse • Sexual abuse • Emotional/psychological abuse • Financial or material exploitation • Abandonment • Neglect • Self-neglect
Physical Abuse • The use of physical force that might result in bodily injury, physical pain, or impairment. • Most readily substantiated form of abuse • Example: Mr. Smith is Mrs. Smith’s caregiver. Frustrated by Mrs. Smith’s refusal to bathe, Mr. Smith finally forces her into a bath and holds her there to clean her, resulting in bruises on her arms.
Sexual Abuse • Nonconsensual sexual contact of any kind with an older person. • Example: Mr. Jones, a midely demented resident in a supported housing complex mistakes Mrs. Doe, another resident, for his wife, and is found one afternoon lying on top of her in her bed and stroking her.
Emotional Abuse • The infliction of anguish, pain, or distress • Example: Bill lives with his daughter, Susan, who provides him care. However, Susan constantly reminds Bill of the sacrifices she makes for him, tells him that he is ruining her life, and complains that he is a chore and a burden for her.
Financial Exploitation • The illegal or improper use of an older person’s funds, property, or assets. • Example: In exchange for providing his mother with care, a son insists that she buy him alcohol and cigarettes, not leaving her enough money to pay for all of her medications.
Abandonment • The desertion of an older person by an individual who had physical custody or otherwise had assumed responsibility for providing care for an older person. • Example: Susan gets so frustrated with her demanding, agitated, father, that she storms out of the house one weekend for a “break,” leaving him completely alone and unsupervised for a number of days.
Neglect • The refusal or failure to fulfill any part of a persons obligations or duties to an older person The most difficult form of abuse to validate • Example: Glenda is attempting to care for her frail mother while also caring for her four young children. Glenda is so busy with her children and home that her mother often goes unchanged after episodes of incontinence, resulting in a sacral ulceration.
Self-Neglect • The behaviors of an older person that threaten his/her own health or safety. • Example: Beth tries to convince her father, John, to move into assisted living after he is diagnosed with early Alzheimer’s disease. He refuses, and when she finally visits him to speak to him in person, she finds him sitting alone in his house, physically weak and covered in filth. The house is filled with garbage and half-eaten meals, and infested with roaches.
Prevalence of specific types of abuse Neglect 48.7% Psychological 35.4% Financial 30.2% Physical 25.6% Abandonment 3.6% Miscellaneous 1.4% Sexual 0.3%
Risk Factors for Abuse • Substance abuse history by the caregiver • Most likely alcoholism • Incidence of addiction in an abuser is 35% • Older age • Elderly in the >80 age group are 2-3 times more likely to be abused or neglected. • History of depression or mental illness of the care recipient • Occurs in 45-50% of victims
Risk Factors Continued • Low income • Social isolation • Minority status • Low level of education • Previous history of family violence
Caregiver Burnout? • Caregiver depression is sited as a separate risk factor for abuse. • Perception of stress by the caregiver was correlated with increased abuse. • Victim’s aggressive behavior toward caregivers has been shown to increase the probability of physical abuse.
Recognizing the Abuser • 47% of abuse cases are committed by the spouse. • 19% of abuse cases were committed by the adult child. • Males abuse more often than females. • Caregiver dependence on the victim for financial assistance, housing, or other needs increases the risk for abuse. • Alcohol abuse is the most common risk factor for physical abuse. • A poor relationship between caregiver and care recipient is a predictor of stress that leads to abuse.
Recognizing the Abused Suspicious factors: • Frequent admissions to multiple hospitals • Surgeries secondary to trauma • Irregular medical follow-up • Inattention to established medical needs • Missed appointments • Unfilled prescriptions • Multiple, vague, complaints
Physical signs of abuse • Poor hygiene • Poor nutrition • Poor skin integrity • Contractures • Pressure ulcers • Dehydration • Impaction • Malnutrition • Inappropriate dress • Unexplained bruises • Restraint marks on wrists • Lacerations • Abrasions • Head injury • Unexplained fractures • Bite marks • Inguinal rash • Genital pain, itching
Medical Implications of Abuse • Reduced quality of life of abused patients • Worsened functional status • Progressive dependency • Poorly rated self-health • Feelings of helplessness • Continued and worsened social isolation, stress and further psychological decline • Frequent ER visits • Higher rate of hospitalization of abused • Higher nursing home placement • Abuse is an independent predictor for higher mortality. • Abused are 3 times more likely to die.
Why Health Care Providers Don’t Ask • Lack of training in recognizing abuse • Lack of time in office to deal with issues • Reluctance to attribute signs of mistreatment • Victim isolation • Subtle presentations • Reluctance in confronting the offender • Reluctance to report if abuse is only “suspected” • Lack of knowledge of how to report • Empathy with abuser • Request of victim
How to Ask • Interview should be conducted privately. • Should take the form of dialogue when possible. • Make questions a “routine” part of the interview. • Document answers meticulously, using interviewees own words whenever possible.
Screening Questions • Has anyone ever touched you without your consent? • Has anyone ever made you do things you didn’t want to do? • Has anyone taken anything that was yours without asking? • Has anyone ever hurt you? • Has anyone ever scolded or threatened you? • Have you ever signed documents you didn’t understand? • Are you afraid of anyone at home? • Are you alone a lot? • Has anyone ever failed to help you take care of yourself when you needed help?
Health Care Professional Responsibilities • To recognize or suspect abuse and neglect when present. • To treat any medical problems associated with such maltreatment. • To ensure a safe disposition for the patient.
How to Report • Call Seniors Abuse Line:1 888 896-7183In Winnipeg:(204) 945-1884 • Age & Opportunity Confidential Intake Line:(204) 956-6440 • Protection for Persons in Care Office:1 866 440-6366To report abuse in care facilities:(204) 788-6366 in Winnipeg
Summary • Abuse is a very prevalent problem among the quickly expanding geriatric population. • Recognition of risk factors for abuse will help the health care provider to know when to further question patients for signs of abuse. • Only through awareness and a healthy suspicion can you detect mistreatment. • Older people often rely on their the health care provider to help in dealing with abuse. • Once it is reasonably suspected, elder mistreatment should be reported to the appropriate authorities
Be Part of the Solution www.olderadultabuse.mb.ca Organize an event for World Elder Abuse Awareness Day June 15 - Wear purple