Plethysmography
Plethysmography. Standard PF Plethysmograph. Spirometry Spirometry Diffusion Capacity Diffusion Capacity Lung Volumes Lung Volumes MIP/MEP MIP/MEP Thoracic Gas Volume Airways Resistance. Myths. Plethysmography is too difficult for the patient.

Plethysmography
E N D
Presentation Transcript
Standard PF Plethysmograph • Spirometry Spirometry • Diffusion Capacity Diffusion Capacity • Lung Volumes Lung Volumes • MIP/MEP MIP/MEP Thoracic Gas Volume Airways Resistance
Myths Plethysmography is too difficult for the patient. Plethysmography is too expensive Plethysmography is too complex and useful only as a research tool. My it will be torture for my patients 3
What does it measure? Flow (Volume) Mouth Pressure Box Pressure 6
How does it measure? Mouth Pressure Xducer Pneumotachometer (Flow) Box Pressure Transducer
How Does It Work? As the patient pants against the closed shutter, pressure change is measured in the box and at the mouth 8
Assumptions Mouth Pressure (Pm) is equal to alveolar pressure (Palv) Abdominal gas does not effect the measurement 9
How Does It Work? Pascal’s Principle P1 • In a fluid or gas filled circuit, pressure applied at any point is felt equally throughout the circuit • This assumption must be true for results to be valid P3 P2 10
Why Calculate lung volumes • A restrictive ventilatory defect is characterized by a reduction in TLC • below the 5th percentile of the predicted value • Below the lower limits of normal
Why Determine Lung Volumes ERS/ATS: The presence of a restrictive ventilatory defect may be suspected when VC is reduced. A reduced VC by itself does not prove a restrictive ventilatory defect. 12
Why Determine Lung Volumes ERS/ATS: A reduced FVC is associated with a low TLC only 50% of the time or less. 13
Lung Volumes • Thoracic Gas Volume (TGV) also called FRCpleth – the volume of air in the lungs at the end of a normal exhalation • We are after Total Lung Capacity (TLC); however, TLC is not measured directly. 14
Lung Volumes • TLC = TGV (FRC) + Inspiratory Capacity (IC) • TLC = Residual Volume (RV) + VC • RV = TGV - ERV 15
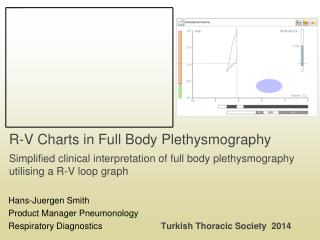
Lung Volumes 16
Determination of FRC • Multiple breath gas dilution • Nitrogen Washout • Helium Dilution • TGV via Body Plethysmography • Imaging Techniques (radiology) • Planimetry • CT/MRI
Determination of FRC ACCP Scientific Section Recommendation: In patients with airway obstruction the dilution method underestimates the thoracic gas volume to the extent that depends on the severity of the obstruction. The plethysmographic method measures the total compressible gas including that of poorly ventilated areas. Murray, Crapo, et al ,1982 18
Determination of FRC • Dilution methods measure onlycommunicating airways and therefore can significantly underestimate true lung volume.
FRC by Plethysmography = 2L FRC by Dilution = 2L
Obstructed airway FRC by Dilution = 1 L FRC by Plethysmography = 2L
Determination of TLC via Single Breath Single breath inert gas dilution (DLco) Helium, Neon, Methane Alveolar Volume (VA) approximates TLC Single breath techniques further underestimate lung volume due to reduced time for equilibration. 22
Plethysmography vs. Dilution Decreases test time – One N2 washout or helium dilution can take up to 7-8 minutes. If you have to repeat, this takes an additional 7-8 minutes after waiting for gas to clear lungs Plethysmography can perform several efforts in 3 minutes 23
Clinical Indications To distinguish between restrictive and obstructive disease patterns, particularly in the presence of a reduced VC To diagnose restrictive disease patterns To provide an index of gas trapping (plethysmographyvs gas dilution) Assess response to therapeutic intervention AARC Clinical Practice Guideline 24
TGV - How Does It Work? P P` • Boyle’s Law • P1V1 = P2V2 V` V
TGV - How Does It Work? • P1V1 = P2V2 • P1 = barometric Pressure* • V1= thoracic gas volume • P2 = P1 + delta P • V2 = V1 - delta V • Solving for P1 • V1 = PB • (V / P) 26
Testing Sequence(1st Choice) • Measure ERV after the acquisition of the FRC measurement followed by slow IVC maneuvers that are linked • FRC reported – mean of technically acceptable FRC measurements (CV 5% = difference between highest and lowest values divided by the mean ≤ .05) linked to technically acceptable ERV and IC measurements used for calculating RV and TLC • Acceptable IC’s CV 5% +/- 3% (obstructed)
Testing Sequence 2nd Choice • Perform IC immediately after the FRC measurement to TLC • This method might work better for those who have severe COPD • TLC = FRC + IC
Airways Resistance (Raw)
Airways Resistance (Raw) Airways Resistance can be thought of as how much work (driving pressure) the patient has to do simply to breath. 31
Airway Resistance (Raw) • Increased Raw is the primary finding in Obstructive Airways Disease • May be caused by bronchospasm, compression or consolidative filling 32
Airways Resistance (Raw) Airways Resistance - Pressure cmH2O/L/sec Conductance (Gaw) – Flow L/sec/cmH20 Gaw is the reciprocal of Raw 1/Raw 33
Airways Resistance (Raw) Airways Resistance - Pressure cmH2O/L/sec sRaw (Raw relative to lung volume) Raw x Vpant Conductance (Gaw) – Flow L/sec/cmH20 sGaw (Gaw relative to lung volume) Gaw/Vpant 34
Airways Resistance (Raw) COPD patient - Raw sRaw sGaw Compensatory Hyperinflation 35
Airway Resistance Effort independent assessment of airway caliber ! If pressure is constant which will conduct more flow?
Poiseuille’s Law (Pdriving)(pi)(radius4) Flow = ------------------------- (8)(Length)(viscosity) Flow rate is proportional to the 4th power of a pipe’s radius. 37
Poiseuille’s Law You need 16 tubes to pass as much fluid as one tube twice their diameter. 38
Airway Resistance • Since resistance is related most strongly to total cross sectional area rather than length, the majority of resistance in normal lungs resides in the larger airways P1 P2 P3B P3A P3B2 P3A1 P3B1 P3A2
Airways Resistance • In summary, what proportion of the total airways resistance is in the larger airways? • What proportion of the airways resistance is in the smaller airways? • 80% Larger • 20% Smaller
Pleth Test Maneuver Door closed for ~1 min to allow for equilibration Patient sitting up straight, nose clips Hands supporting their cheeks Elbows at their side 41
TGV Test Maneuver Normal tidal breathing until stable respiratory pattern is achieved At end expiration the shutter is closed Patient is asked to “pant” against the closed shutter for 2 to 3 seconds. After shutter reopens, perform an SVC 42
Thoracic Gas Volume – “Panting” • Pant Volume: ~50cc • Frequency: 0.5 – 1.0 Hz (30 to 60 bpm, although up to 90 is acceptable) • Emphasize this is NOT an MVV or MIP/MEP
Thoracic Gas Volume – “Panting” Tidal Breathing Shutter Closure 44
How Does It Work? Mouth Pressure vs Box Pressure Mouth Pressure Box Pressure (pleth volume)
How Does It Work? Mouth Pressure Box Pressure (pleth volume) V / P is the relationship between mouth pressure and box pressure, and can be expressed as the tangent of the angle 46
Importance of “pinned” SVC • Trying to measure TLC • TGV efforts can be variable • Performing an SVC with the TGV maneuver produces more repeatable TLC values
Airway Resistance Test • Open Shutter Phase • Pant with shutter open to determine airway resistance • Closed Shutter Phase • Pant with shutter closed to measure lung volume – VPant (can be used to measure TGV)